Full implementation of CT lung cancer screening in the U.S. could save more than 12,000 lives each year, even if the relatively conservative criteria of the National Lung Screening Trial (NLST) are used, according to a new study in Cancer. The study is one of the first to set a definitive value on the potential benefits of CT screening.
Among the approximately 8.6 million screening subjects in the U.S. who fell within the screening guidelines, 8,990 deaths among men and 3,260 deaths among women would be averted each year, concluded Jiemin Ma, PhD, and colleagues from the American Cancer Society.
The implementation of low-dose CT (LDCT) screening among individuals eligible under the NLST criteria would avert approximately 7.6% of total annual lung cancer deaths, the researchers wrote (Cancer, February 25, 2013).
Results from NLST, published in 2011, demonstrated that low-dose CT screening could reduce deaths by up to 20% compared to chest radiography in a population of smokers ages 55 to 74 years, who had a smoking history of at least 30 pack-years or, if no longer smoking, had quit within the past 15 years.
In the Cancer study, the researchers estimated the number of lives that would be saved annually if NLST-based screening guidelines were fully implemented in the eligible U.S. population. Of course, full implementation of screening would also require money that Congress has not yet allocated, so the authors also performed a brief literature review to evaluate cost-effectiveness as well.
"There are no data that provide national estimates on the impact of implementing the findings of the National Lung Screening Trial, so we wanted to apply these estimates," said study co-author Ahmedin Jemal, PhD, vice president of surveillance research, in an interview with AuntMinnie.com. "We wanted to fill in the gap with that information."
The study team estimated the number of avoidable cancer deaths via a formula that included age groups (55-59 years, 60-64 years, 65-69 years, and 70-74 years), gender, smoking status, mortality rate, and effect of screening on lung cancer mortality -- assumed to be a 20% benefit across the board.
The group used 2010 U.S. Census data for age- and sex-specific population estimates, estimating the prevalence of screening eligibility among the 7,138 participants in the 2010 National Health Interview Survey (NHIS). NHIS-linked mortality files for smokers were then used to estimate mortality from 2000 through 2004, and this group was followed for an additional two years. For those smokers eligible for screening, the group derived lung cancer mortality rates using the rates for eligible current smokers, as well as those for eligible smokers who had quit.
Among the eligible population, "if all those men and women were to receive screening, we would avert about 12,000 deaths," or 7.6% of the estimated 160,000 annual lung cancer deaths in the U.S., Jemal said.
Broken down by gender, the results showed that about 5.2 million men and 3.4 million women were eligible for lung cancer screening in 2010, and among the total 8.6 million, 12,250 deaths would be avoided each year.
| No. of cancer deaths averted per year with LDCT | |||||
| Age | Male (n) | Female (n) | Total (n) | ||
| Current smokers | |||||
| 55-59 | 719 | 353 | 1,072 | ||
| 60-64 | 1,599 | 296 | 1,895 | ||
| 65-69 | 1,643 | 545 | 2,188 | ||
| 70-74 | 912 | 654 | 1,566 | ||
| Former smokers | |||||
| 55-59 | 421 | 176 | 597 | ||
| 60-64 | 834 | 139 | 973 | ||
| 65-69 | 1,516 | 636 | 2,152 | ||
| 70-74 | 1,346 | 461 | 1,806 | ||
| Total | 8,990 | 3,260 | 12,250 | ||
Acknowledging that screening 100% of the eligible population isn't likely, the authors stated that screening even a fraction of the population could significantly affect mortality.
The 12,250 estimate was based on a 20% reduction in deaths and 100% utilization of screening, but the group also looked at the impact of 15% and 30% mortality reductions in various percentages of the population.
"Under the optimal scenario (100% screening uptake rate and a 30% reduction in lung cancer death rates), the number of lung cancer deaths averted by LDCT screening is 18,375," Ma and colleagues wrote. "If 70% of the 8.6 million eligible people are screened annually, there would be 8,575 lung cancer deaths averted by LDCT screening."
Research needed on costs
But how much would such a screening program cost, if implemented on a national scale?
"We haven't really addressed the costs, but estimates are everywhere in the literature," Jemal said.
Estimates cited in the study ranged from the $240,000 to avert one cancer death estimated by Goulart et al, down to $2,500 -- the cost of a single scan -- as the minimum cost to save the same life by Henschke et al in the Early Lung Cancer Action Program (ELCAP). McMahon et al estimated the cost of an additional quality-adjusted life year (QALY) at $126,000 to $169,000, while Pyenson et al came in at a more modest $19,000 per QALY. "I think that's probably an area that has to be looked at very carefully," Jemal said.
Despite the varying cost estimates, Jemal believes the Cancer study demonstrates the value of CT lung cancer screening in terms of lives saved.
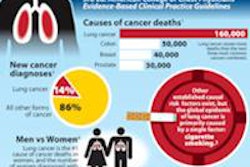
"When you look at 12,000 cases a year, that's a lot," Jemal said. With a toll estimated at 160,000 deaths a year, lung and bronchial cancers dwarf all other cancers as a cause of death, he said.
However, other factors might have affected the study's estimates of cancer deaths averted, the authors cautioned. For one thing, the NLST control group received chest x-rays, while most of the at-risk population in the U.S. would likely receive no screening. This could lead to an underestimation of lives saved with low-dose CT. In addition, the lung cancer mortality rates in the study were based on deaths that occurred between 2000 and 2006, possibly overestimating current mortality rates.
"Further studies are needed to estimate the number of avertable lung cancer deaths and the cost-effectiveness of LDCT screening under different scenarios of risk, various screening frequencies, and various screening uptake rates," Ma and colleagues concluded.