An MR "fingerprinting" approach could help better assess prostate cancer, suggest findings published April 7 in Radiology.
Researchers led by Dheeman Futela, MBBS, from Case Western Reserve University in Cleveland, developed a rapid, B1-insensitive MR fingerprinting technique for focal prostate lesion characterization. They reported success from this approach, especially when combining apparent diffusion coefficient (ADC) and MR fingerprinting T2 imaging.
“Quantitative MRI evaluation of prostate lesions using rapid, B1-insensitive prostate MR fingerprinting and apparent diffusion coefficient mapping differentiated clinically significant cancers from clinically insignificant lesions,” Futela and colleagues wrote.
MR fingerprinting is a quantitative technique that allows for simultaneous quantification of T1 and T2 images. Earlier studies have shown that T1 and T2 relaxometry derived from MR fingerprinting can differentiate prostate lesions, especially when combined with ADC mapping.
In MRI, the B1 field is the radiofrequency pulse used to tip protons out of alignment so they can be detected. At higher field strengths, the B1 field becomes more uneven, affecting image quality.
Futela and co-authors designed a B1-insensitive MR fingerprinting technique with an acquisition speed of 15 seconds per section. They previously showed this technique led to a day-to-day variation of less than 3% in T1 and T2 assessment for kidney imaging.
The researchers tested this approach on focal prostate lesion characterization in the peripheral zone. They used MRI-guided transrectal ultrasound fusion biopsy-derived histopathologic analysis as the reference standard.
The study included 52 male patients with an average age of 65 years who had 51 peripheral zone prostate lesions. All lesions were scored as PI-RADS 3 or above.
The mean T2 and ADC were lower for clinically suspicious prostate cancer (n = 22) than for clinically insignificant lesions (n = 29).
Mean T2, ADC for clinically suspicious and insignificant prostate lesions | |||
Measure | Clinically insignificant | Clinically suspicious | P-value |
T2 | 80 msec | 56 msec | < 0.001 |
ADC | 876 × 10−6 mm2/sec | 668 × 10−6 mm2/sec | < 0.001 |
At univariable analyses, an optimal T2 cutoff of 58 msec achieved an area under the curve (AUC) of 0.87. This included a sensitivity of 73% and a specificity of 93%. And an ADC cutoff of 761 × 10−6 mm2/sec led to an AUC of 0.83 (82% sensitivity; 79% specificity).
A multivariable model incorporating both T2 and ADC achieved a higher performance (AUC 0.90; p < 0.001). The researchers also highlighted further improvement in diagnostic performance when serum prostate-specific antigen density (PSAD) was included (AUC, 0.94; p = 0.01).
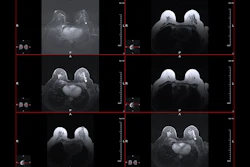
 Representative T2-weighted (T2w) images, apparent diffusion coefficient (ADC) maps, and MR fingerprinting (MRF)-derived T1 and T2 maps obtained from three participants with different histologic types of prostatic lesions. Lesions are circled with dashed lines. Mean values with standard deviations for ADC, T1, and T2 are shown at the bottom of the images. PCa = prostate cancer.RSNA
Representative T2-weighted (T2w) images, apparent diffusion coefficient (ADC) maps, and MR fingerprinting (MRF)-derived T1 and T2 maps obtained from three participants with different histologic types of prostatic lesions. Lesions are circled with dashed lines. Mean values with standard deviations for ADC, T1, and T2 are shown at the bottom of the images. PCa = prostate cancer.RSNA
The study authors called for future studies with a larger sample size and multi-institutional datasets to confirm these findings and refine multiparametric MRI interpretation.
The results add to the conversation on incorporating quantitative imaging in the next generation of prostate cancer detection, according to an accompanying editorial written by Daniel Margolis, MD, from Weill Cornell Medicine in New York and Vikas Gulani, MD, PhD, from the Michigan Institute of Imaging Technology and Translation in Ann Arbor.
Despite the limitations of the study, Margolis and Gulani suggested that a combination of quantitative techniques and AI will “likely succeed” with the current qualitative system.
“Quantitative and reproducible methods such as MR fingerprinting are likely more conducive to a formula-based score, and the inherent co-registration of MRI fingerprinting means that incorporation of multiple quantitative metrics may be feasible,” they wrote. “Time added to scanning and billing considerations add further complexity to the adoption of quantitative imaging in prostate evaluation.”
Read the full study here.