Ultrafast breast MRI can differentiate between markers tied to malignancy, according to research published April 9 in the American Journal of Roentgenology.
A team led by Helaina Regen-Tuero, MD, from NYU Langone Health in New York City found that earlier visualization of a focus relative to background parenchymal enhancement (BPE) on ultrafast MRI is tied to a higher risk of malignancy. However, morphologic features showed no association with malignancy.
"In other words, if a focus enhanced earlier than the surrounding parenchyma, it was more likely to be malignant," Regen-Tuero told AuntMinnie. "If a focus enhances notably earlier than the surrounding parenchyma on ultrafast MRI, it may warrant closer attention or biopsy."
Breast MRI is ideal for finding small cancers, but differentiating benign from malignant lesions is still challenging. The researchers pointed out that this especially goes for foci, tiny spots of enhancement found on MRI. In rare cases, foci may represent early signs of breast malignancy.
Regen-Tuero and colleagues evaluated whether kinetic features on ultrafast MRI can determine malignant from benign foci.
The single-center retrospective study included ultrafast MRI exam data collected between 2019 and 2023. The research team included exam data from 124 women who underwent MRI-guided biopsy for 124 foci. It also calculated the difference between time to enhancement (TTE), focus, and BPE.
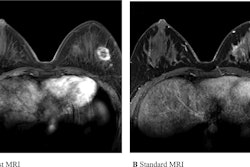
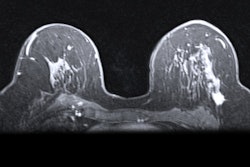
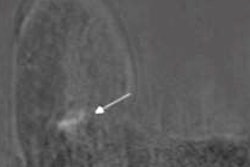
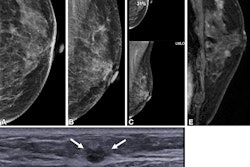
 (A) Ultrafast MR image obtained 14 seconds after aortic enhancement shows 0.4-cm focus (arrow) in the left breast at 3-o’clock position, 4.5 cm from index cancer (not shown). (B) Ultrafast MR image obtained 23 seconds after aortic enhancement shows wash-in (arrow) of background parenchymal enhancement (BPE). (C) and (D) On first standard postcontrast subtraction MR images, focus (arrow, C) and BPE (arrow, D) are indistinguishable. MRI-guided biopsy of focus yielded grade 2 invasive lobular carcinoma. Image courtesy of the ARRS.
(A) Ultrafast MR image obtained 14 seconds after aortic enhancement shows 0.4-cm focus (arrow) in the left breast at 3-o’clock position, 4.5 cm from index cancer (not shown). (B) Ultrafast MR image obtained 23 seconds after aortic enhancement shows wash-in (arrow) of background parenchymal enhancement (BPE). (C) and (D) On first standard postcontrast subtraction MR images, focus (arrow, C) and BPE (arrow, D) are indistinguishable. MRI-guided biopsy of focus yielded grade 2 invasive lobular carcinoma. Image courtesy of the ARRS.
Of the total women in the study, 64 were postmenopausal, 71 had a personal history of breast cancer, 81 had a family history of breast cancer, and 33 had genetic mutations. Also, 59 of the total exams performed were for extent of disease evaluation while 52 were for screening purposes. Seventy-two of the women had heterogeneous fibroglandular tissue while 71 had mild BPE.
Of the 124 foci included, 21 were malignant, 16 were invasive, and five were ductal carcinoma in situ (DCIS).
The researchers reported the following:
- Malignancy risk increased by 5% with each one-second increase in the difference of lesion TTE and BPE TTE (p = 0.006).
- Older age and lower BPE were significantly associated with increased likelihood of malignancy (p = 0.005 and 0.02, respectively).
- Odds of malignancy for women with minimal or mild BPE were 11.7 times the odds of those with moderate or marked BPE.
- No other demographic or lesion characteristics were tied to malignancy.
The difference of focus TTE and BPE TTE could help classify foci as malignant or benign, the researchers explained.
Regen-Tuero said that "surprisingly," while prior studies looking at other lesion types have shown shorter TTEs are associated with increased likelihood of malignancy, TTE of the focus alone in this study was not predictive of malignancy. This may have to due with the small size of the lesions the researchers evaluated, she added.
"Additionally, while higher levels of BPE are generally thought to be associated with increased cancer risk, our study found that lower levels of BPE were actually associated with higher odds of a focus being malignant, possibly due to better lesion conspicuity against a quieter background," she told AuntMinnie.
The study authors called for future studies to evaluate how well this classification works in independent sets of women and determine a threshold TTE difference leading to maximum specificity and sensitivity measures.
The full study can be found here.