Age-adjusted breast arterial calcifications (BACs) from mammograms can predict cardiovascular events beyond traditional risk scores, according to research published April 24 in JACC: Cardiovascular Imaging.
An AI model showed success in a study by reclassifying low- and intermediate-risk women based on their age-adjusted BACs, wrote a team led by Nitesh Nerlekar MBBS, PhD, from Victorian Heart Hospital in Melbourne, Victoria, Australia.
“Integration of BAC into cardiovascular risk assessment frameworks may facilitate early identification of at-risk women,” the Nerlekar team wrote.
BACs in recent years have become more recognized as a risk factor for later cardiovascular events in women, leading to more interdisciplinary collaboration between radiologists and cardiologists. However, the researchers noted that classifying BAC findings is limited by subjective radiologist grading and inconsistent reporting patterns.
Nerlekar and colleagues developed an age-adjusted BAC percentile nomogram from screening mammograms to study associations between age-adjusted BAC percentiles and major adverse cardiovascular events (MACE). They also evaluated the incremental predictive value of BAC percentiles beyond atherosclerotic cardiovascular disease (AVSCD) risk categories and the impact of BAC percentiles on risk reclassification, calibration, and clinical use.
Finally, the researchers also developed a complementary online calculator tool that shows how BAC percentiles support decision-making.
The multicenter, retrospective cohort study included 21,514 women with no known cardiovascular disease and who were 40 or older. These included women at sites based in the U.S. and Australia who underwent screening mammography and ASCVD risk assessment. The researchers quantified BAC by using an AI model (cmAngio research edition, CureMetrix) for age-adjusted percentiles.
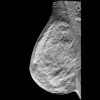
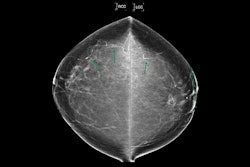
 Example of Percentile Nomogram With Age-Adjusted BAC Quartiles. (A) Mammogram of a 56-year-old woman. There is evident BAC (pink arrow). This was quantified as a BAC score of 30 using the cmAngio tool. (B) Nomogram indicating that a BAC score of 30 places a 56-year-old woman within the 50th to 75th percentile for her age. Images are republished under a Creative Commons license (CC BY 4.0).JACC: Cardiovascular Imaging
Example of Percentile Nomogram With Age-Adjusted BAC Quartiles. (A) Mammogram of a 56-year-old woman. There is evident BAC (pink arrow). This was quantified as a BAC score of 30 using the cmAngio tool. (B) Nomogram indicating that a BAC score of 30 places a 56-year-old woman within the 50th to 75th percentile for her age. Images are republished under a Creative Commons license (CC BY 4.0).JACC: Cardiovascular Imaging
Of the total women, 22.7% had BACs present on mammography. This increased with age, with 61% of women over the age of 70 having a BAC compared to 8% of women younger than 50 years. And during an average follow-up of 4.7 years, 828 MACEs (3.8%) occurred.
Each 10-percentile increase in BAC was tied to a 17% relative increase in MACE risk (adjusted HR [aHR]: 1.17; p < 0.001), independent of conventional risk factors.
Women with low ASCVD risk (80% of cohort) had significantly increased MACE with both BAC percentile less than median (aHR: 1.66; p < 0.001) and more than median (aHR: 2.31, p < 0.001). Women with intermediate and high ASCVD risk had greater MACE when BAC was more than median (intermediate aHR: 1.40, p = 0.01; high aHR: 1.65, p < 0.001).
Adding BAC to ASCVD risk scoring appropriately up-classified 9% of individuals with MACE and down-classified 3% of individuals without events. This led to an overall net reclassification index of 5%. Finally, adding BAC to risk scoring led to an improved ability to rank patients from high to low risk (C-statistic) from 0.67 to 0.71 (p = 0.04).
The results support integrating BAC assessment into routine mammographic workflows to improve cardiovascular risk stratification in women, the study authors wrote.
“By leveraging widely available imaging and AI–based automation, BAC percentile scoring offers a personalized, noninvasive tool for identifying at-risk individuals who may otherwise remain unrecognized in primary prevention frameworks,” they wrote.
The authors are affiliated with CureMetrix, which provided the software used in the study. Read the full study here.