MRI-guided microwave ablation of small liver tumors near the diaphragm or heart achieved zero local recurrence over nearly three years of follow-up, according to a poster to be presented May 11 at the ISMRM meeting in Cape Town, South Africa.
The findings suggest that real-time MRI guidance may offer safety and precision advantages over conventional imaging for these tumors, noted lead author Daniel Dux, MD, of Hannover Medical School in Germany, and colleagues.
“[MRI-guided microwave ablation] is a feasible, safe, and effective minimally invasive treatment for small subdiaphragmatic and pericardial liver tumors, providing excellent local tumor control and a manageable complication profile,” the group wrote.
Microwave ablation (MWA) is an increasingly accepted minimally invasive treatment for small hepatic malignancies because it offers comparable oncologic outcomes to surgery with lower morbidity, according to the authors. However, tumors in subdiaphragmatic or pericardial locations pose technical challenges due to limited access and cardiac/respiratory motion, increasing risk of incomplete treatment and complications, they noted.
MRI's superior soft-tissue contrast and real-time multiplanar imaging capability offer a potential alternative, though data on its use in this specific subset of patients remain limited, the group added.
To bridge the gap, the researchers reviewed consecutive MRI-guided microwave ablation procedures performed at their hospital between February 2017 and May 2025 on a 1.5-tesla system with a 70 cm bore. The study included 23 patients who underwent ablation for 25 tumors: 20 subdiaphragmatic and five pericardial. All tumors measured 2 cm or less (mean lesion diameter, 13.1 mm) and were located within 10 mm of the diaphragm or heart.
According to the results, technical success was 100%. Mean total procedure time was two hours and 14 min ± 51 min. Over a mean follow-up of 32.5 months, no local tumor progression or recurrence was detected in any of the 21 patients with post-treatment imaging.
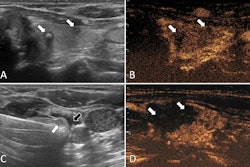
 A and B: T1-weighted MRI (portal venous phase) show a 16 mm hepatic metastasis (red arrow), with a minimum distance of 0 mm to the diaphragm. D and E: Immediate post-ablation T1-weighted MRI (portal venous phase) in reformatted orientation along the antenna trajectory (green arrow) demonstrates complete tumor necrosis. C and F: CT images (portal venous phase) acquired 20 months post-ablation reveal the remaining ablation zone without evidence of residual/recurrent tumor.Daniel Dux, MD, and ISMRM
A and B: T1-weighted MRI (portal venous phase) show a 16 mm hepatic metastasis (red arrow), with a minimum distance of 0 mm to the diaphragm. D and E: Immediate post-ablation T1-weighted MRI (portal venous phase) in reformatted orientation along the antenna trajectory (green arrow) demonstrates complete tumor necrosis. C and F: CT images (portal venous phase) acquired 20 months post-ablation reveal the remaining ablation zone without evidence of residual/recurrent tumor.Daniel Dux, MD, and ISMRM
"MRI guidance likely contributed to safety advantages by enabling real-time, multiplanar visualization and precise craniocaudal antenna trajectories that avoid transpleural approaches and associated pulmonary complications," the authors wrote.
Limitations included the study’s retrospective design, single‑center experience, small sample size -- particularly for pericardial lesions -- and two patients without follow‑up, the group noted.
“Our findings require validation in prospective, multicenter and comparative studies (CT/US guidance or surgery) to refine patient selection and generalizability,” the authors concluded.