Technetium-99m-Tetrofosmin Tumor Imaging:
Lung Cancer:
The multi-drug-resistant energy dependent P-glycoprotein pump system (MDR-Pgp) may play a role in the resistance of lung cancer to certain chemotherapeutic agents. Determination of MDR-Pgp at time of diagnosis may provide information regarding which treatment protocol would be best for each individual patient. P-glycoprotein recognizes certain chemotherapy agents as substrates (such as paclitaxel- a taxane agent) and is involved with their transport out of the cell. P-glycoprotein also works to prevent intracellular accumulation of some lipophilic cationic radiopharmaceuticals such as Tc-Tetrofosmin. Cancers with low uptake of Tc-Tetrofosmin likely have overexpression of MDR-Pgp and are more likely to be associated with a poor response to certain chemotherapy agents [4].
Thyroid cancer:
Tetrofosmin [1,2-bis-(bis[-2-ethoxyethyl) phosphino] ethane] is a lipophilic cationic complex which passively diffuses across cell membranes. The tumor uptake mechanisms and intracellular binding mechanisms have not been completely described but is likely dependent on blood flow and transmembrane and mitochondrial potentials [1]. The agent has been used for the detection of recurrent disease and metastatic lesions in patients being followed for thyroid cancer. Similar to thallium and sestamibi, patients do not need to discontinue thyroid replacement therapy prior to the scan. Non-iodine avid metastases have been demonstrated with Tc-99m-tetrofosmin. Overall sensitivity for detection of distant metastatic lesions is 85-88%. Uptake in the non-malignant thyroid remnant can occur in up to 67% of cases and can make differentiation from local tumor recurrence difficult. However, other authors report poor sensitivity (33%) for the detection of residual non-malignant thyroid tissue [5].
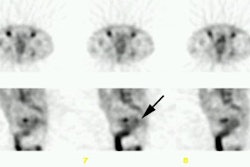
Early abdominal imaging (as soon as 5 minutes post-injection) is necessary for lesion detection as gut and biliary activity rapidly obscure detail in this region. Similr to thallium, pulmonary metastases may not be identified [3]- SPECT imaging may aid in detection of pulmonary lesions [5]. The agent is less sensitive for the detection of osseous mets [1,2]. Unfortunately, tetrofosmin uptake is not specific for thyroid cancer and does not give predictive information on the therapeutic potential of I-131. The agent may best be utilized in patients with elevated thyroglobulin levels, but negative radioiodine scans or in combination with radioiodine scanning [3].
REFERENCES:
(1) J Nucl Med 1997; Lind P, et al. Technetium-99m-tetrofosmin whole-body scintigraphy in
the follow-up of differentiated thyroid cancer. 38: 348-352
(2) J Nucl Med 1998; Gallowitsch HJ, et al. Thyroglobulin and low-dose iodine-131 and technetium-99m-tetrefosmin whole-body scintigraphy in differentiated thyroid carcinoma. 39: 870-875
(3) J Nucl Med 1998; Unal S, et al. Thallium-201, Technetium-99m-tetrofosmin and Iodine-131 in detecting differentiated thyroid carcinoma metastases. 39: 1897-1902
(4) J Nucl Med 2001; Kao CH, et al. Paclitaxel-based chemotherapy for non-small cell lung cancer: Predicting the response with 99mTc-tetrofosmin chest imaging. 42: 17-20
(5) Endocrine and Metabolism Clinics of North America 2001; Haugen BR, Lin EC. Isotope imaging for metastaic thyroid cancer. 30: 469-492