J Am Coll Surg 2000 Nov;191(5):511-8
Can postoperative surveillance with serial CEA immunoscintigraphy detect
resectable rectal cancer recurrence and potentially improve tumor-free survival?
Lechner P, Lind P, Goldenberg DM.
BACKGROUND: This study was performed to determine if postoperative serial monitoring of
rectal cancer patients can be performed with an immunoscintigraphic imaging test for
carcinoembryonic antigen (CEA). It was also of interest to assess whether this test, in
combination with standard monitoring procedures used in an intensive surveillance plan,
can result in the identification of surgically salvageable patients. STUDY DESIGN: Forty
consecutive resected Dukes' B and C rectal cancer patients underwent a prospective,
single-institution, surveillance trial of physical examination (including digital rectal
examination), endoscopy, CT of the abdomen and pelvis, liver ultrasound, chest x-ray,
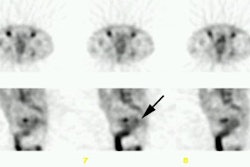
blood CEA, and CEA immunoscintigraphy with arcitumomab (CEA-Scan, Immunomedics, Morris
Plains, NJ) every 6 months for the first 2 years and every 12 months for the next 3 years
after initial operation. Outcomes were compared with those from a similar group of 69
patients treated previously at the same institution but without CEA imaging. RESULTS: A
total of 219 CEA imaging studies were performed without any significant adverse effects or
immune responses, and resulted in lesion sensitivity, specificity, accuracy, and positive
and negative predictive values of 94.1%, 97.5%, 97.3%, 76.2%, and 99.5%, respectively. Of
the 40 patients, 16 developed 22 surgically confirmed local or distant recurrences, and
CEA imaging correctly disclosed 82% of these lesions pre-operatively. All of the patients
found to have recurrences had at least one tumor site by CEA imaging; only 6 of 16 had
elevated blood CEA titers. On a patient-basis, there was a sensitivity of 100%, a
specificity of 79.2%, an accuracy of 87.5%, and positive and negative predictive values of
76.2% and 100%, respectively. The potential therapeutic benefit of serial arcitumomab
imaging is suggested by the fact that 6 of 16 patients (37.5%) with recurrence underwent
potentially curative second-look operations, compared with 6 of 69 (8.7%) of a comparable
population studied at this institution during an earlier 6-year period, using all of the
same tests except CEA imaging. None of the patients in this historic control group
survived more than 21 months, although the mean survival of the six patients resected for
cure in the study population was 35 months (range 11 to 69 months). During 6 years of
followup, three of the six re-resected patients eventually died of cancer recurrence, two
died from other causes (and were confirmed by necropsy to be tumor-free), and one patient
is still free of disease in the sixth year. CEA scanning appeared to be more predictive of
recurrence than blood CEA testing or other diagnostic modalities. CONCLUSIONS: Arcitumomab
inclusion in intensive surveillance of patients with resected rectal cancer can disclose
tumor recurrence at a stage that allowed surgical salvage therapy in 37.5% of the 16
patients with recurrence who had second-look surgery, and in 19% the patients were free of
disease during longterm followup. This pilot study suggests that a randomized prospective
trial comparing standard surveillance procedures to the use of CEA imaging added thereto
should be undertaken.