Dual-energy subtraction chest x-ray edges out conventional imaging because of its ability to detect calcification within a pulmonary nodule. But this technique has its limitations, according to a group from the University of Wisconsin Medical School, Hospital and Clinics in Madison.
Dr. Janet Kuhlman and colleagues outlined the strengths and weaknesses of dual-energy subtraction x-ray in an education exhibit in Radiographics. "Dual-energy subtraction imaging allows better visualization for a variety of entities, including nodules, bone lesions, (and) pleural disease," wrote Kuhlman's group (January-February 2006, Vol.26:1, pp. 79-92).
Of the two types of dual-energy systems available, single exposure and dual exposure, the former suffers from lower signal-to-noise ratio (SNR) of the tissue-selective subtraction image. In contrast, dual exposure produces images with a better SNR by using two sequential x-rays obtained at 60 kVp and 120 kVp to form the standard image.
The trade-off is that dual-energy systems require a slightly higher radiation dose, and can be performed in the posteroanterior view only, which does not obviate the need for lateral imaging, the authors pointed out.
One of the disease entities best visualized with this technique is nodules. Dual-energy subtraction removes overlying bone structures, which can obscure lung nodules.
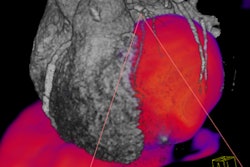
Also, bone lesions, such as primary bone tumors and rib fractures, become more conspicuous. Dual-energy subtraction also improves the visualization of cardiac calcifications and other vascular diseases.
Finally, it can identify pleural calcifications and calcification in pleural plaques, thereby eliminating the need for CT, according to the authors.
There are some pitfalls with dual-energy subtraction imaging. First, the 200-millisecond delay between the two exposures can cause artifacts, which appear as black or white lines, and are most obvious on the bone-selective images. Misinterpretation is another potential hazard as pulmonary nodules are not always identifiable on the tissue-selective image. Misdiagnosing a noncalcified nodule as calcified is another problem.
"Occasionally, a calcium-containing structure can be superimposed on a lung nodule in such a way that the opacity from the calcium appears to be located in the nodule," the authors stated. In addition, motion artifacts around small pulmonary vessels can be mistaken for small calcified nodules.
The authors' final caveats included the following:
- The technique is not suitable for portable chest x-ray
- Dual-energy subtraction imaging should not be performed in the same month as CT
- The technique is not recommended for patients 16 years and younger
They concluded that the ability of dual-energy subtraction imaging to highlight calcifications is its greatest strength, adding that identifying calcification remains essential for characterizing pulmonary nodules.
By Shalmali PalAuntMinnie.com staff writer
February 24, 2006
Related Reading
Chest radiographs negative for one in five acute heart failure patients, January 13, 2006
I-ELCAP data suggest need to work up secondary lung lesions, January 9, 2006
Chest x-ray after thoracentesis adds little new information, December 26, 2005
Lung PET rules when CT is equivocal, discordant, July 12, 2005
Copyright © 2006 AuntMinnie.com