A lack of resolution in the gastric wall layers makes gastric carcinoma staging difficult at best. In Germany, endoscopy with biopsy is the first choice for detecting gastric cancer, but accurate T-staging is not always possible, according to a researcher from the University of Heidelberg. In an effort to give imaging a bigger role in preoperative gastric cancer staging, Dr. Lars Grenacher presented the preliminary results of his group’s work with endoscopic MRI at the 2001 American Roentgen Ray Society meeting in Seattle.
"If you look at five-year cancer survival rates, you can see that for higher stages of gastric cancer, survival is very low," Grenacher said. "For a surgeon, it would be very interesting information to know something about tumor size and growth. If you have a second look at five-year survival rates, for an early cancer with positive lymph nodes (postsurgical treatment residual tumor stage R0), there is a five-year survival rate of 45%. For the same carcinoma at R1, the survival rate is lower than 5%."
For this study, 65 gastric specimens, from humans and pigs, taken after gastroectomy were evaluated in a 1.5-tesla MR unit (Magnetom Symphony, Siemens Medical Solutions, Iselin, NJ). The Heidelberg group also worked with a prototype MR coil designed at the Fraunhofer Institute in St. Ingbert, Germany. Standard MR sequences were used in all possible orientations. The spatial resolution with the coil was 1-5 mm.
"Our intention was to layer discrimination of the gastric wall and to learn something about the morphology of the gastric wall. In addition, we tried to visualize the tumor, and we tried to perform T-staging of these gastric tumors," he said.
 |
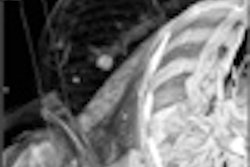
Wall layers visible on MR scans were used to stage gastric cancer. Normal gastric specimens were examined afterwards with an experimental 2.4-tesla MR unit for anatomic correlation. The image above depicts a T3 carcinoma in a human gastric specimen, imaged with the endoscopic MR prototype and confirmed with histologic correlation (Image courtesy of Dr. Lars Grenacher).
According to the results, 96% of gastric carcinomas were seen on the MR scan. Opposed phase imaging was best suited for tumor detection. T2-weighted images were best for wall layer identification. The endoluminal MR coil resulted in the best discrimination of the different gastric wall layers, Grenacher said.
"We could identify up to five layers with our endoluminal MR imaging," he said. "We can see tumors of up to 8 cm up to the gastric wall. This is not possible with endoscopic ultrasound, where only 2-3 mm can be seen."
While T-staging was possible, the accuracy rate for this experimental method was still 50%, Grenacher reported. However, the technique and the equipment show great promise, and the addition of endoscopy could help MRI overcome its limitations for gastric tumor staging.
Other researchers are having similar good fortune with MRI and gastric cancer. A group from St. Mary’s Hospital in Seoul, Korea compared breath-hold 2-D fast low-angle shot (FLASH) and T2-weighted turbo spin-echo fast MR imaging to helical CT in the staging of gastric carcinoma. They found that for T-staging, MRI accuracy was higher than that of helical CT, 73.3% versus 66.7%, although not significantly different from each other (American Journal of Roentgenology, June 2000, Vol.174:6, pp. 1551-1557).
In a second study, also out of Korea, radiologists from Seoul National University College of Medicine evaluated patients with contrast-enhanced CT and a 1-tesla MRI scanner, using FLASH, HASTE, and true-FISP sequences. They found that MRI was slightly superior to CT for T-staging, but that MRI had a tendency to over-stage pathologic T2 cancers (Journal of Computer Assisted Tomography, May-June 2000, Vol.24:3, pp. 389-394).
By Shalmali PalAuntMinnie.com staff writer
July 5, 2001
Click here to post your comments about this story. Please include the headline of the article in your message.
Copyright © 2001 AuntMinnie.com