This article inaugurates a series of white papers on radiologic patient positioning techniques that will appear each month on AuntMinnie.com. The series will explore each of the major modalities. If you'd like to offer your comments or contribute an article, please e-mail [email protected] with your thoughts and suggestions.
Patient preparation
Ask the patient to remove clothes from the waist up, put on a hospital gown, remove any jewelry (necklace, earrings), and, if necessary, tie hair up on top of the head.
For posteroanterior (PA) projections, instruct the patient to sit or stand upright. Patients are positioned to face the film-screen cassette in order to minimize magnification of the anteriorly positioned heart and consequent obscuration of the lungs. Make sure the patient is standing straight and is equally distributing the weight of the body on both feet.
 Posteroanterior (PA) chest projection position, patient against chest board. Image courtesy of Dr. Naveed Ahmad.
Posteroanterior (PA) chest projection position, patient against chest board. Image courtesy of Dr. Naveed Ahmad.The upright position is preferred for the following reasons:
- It prevents engorgement (an excess of blood) of pulmonary vessels, whereas supine or recumbent positioning tends to increase engorgement of pulmonary vessels, which can change the radiographic appearance of these vessels and the lungs.
- It allows full expansion of the lungs. In the recumbent position, full expansion of the lungs is prevented.
- The upright position is very important in order to visualize possible air and fluid levels in the chest. In the upright position, fluid will locate near the base of the lung while the air will rise. In the recumbent position, fluid will spread out over the posterior surface of the lung, resulting in a hazy appearance of the entire lung.
- An upright chest film is preferred over an upright abdominal film for the diagnosis of pneumoperitoneum (free air in the abdominal cavity).
Ask the patient to move the shoulders forward and downward, so that the chest wall and both shoulders are in contact with the cassette. This helps to carry the clavicles below the lung apices.
Adjust the height of the cassette so that its upper border is about 2 inches above the shoulders so that the lung apices are not cut off.
Ask the patient to extend the neck, chin, and head upward and vertical. The neck and chin otherwise tend to superimpose the trachea and uppermost lung regions.
The patient's arms are placed overhead or on their hips with elbows angled anteriorly. This will rotate the scapulae off the chest, thereby preventing their superimposition over the lungs.
In female patients with large pendulous breasts, it is very important to minimize breast shadows. In some patients, depending on the density and size of breasts, breast shadows cannot be totally eliminated. Breast shadows render the examination suboptimal by superimposing over the lower part of the lung fields and obscuring any pathology. Ask the patient to pull the breasts upward and laterally (outwards), then remove her hands as she leans against the cassette holder to keep them in position.
 Breast shadows over lower lung fields. Image courtesy of Dr. Naveed Ahmad.
Breast shadows over lower lung fields. Image courtesy of Dr. Naveed Ahmad.
Place a lead shield between the x-ray tube and the patient's pelvis. Gonadal shielding from the level of the iliac crests, or slightly higher, to the mid-thigh area should be used on all patients of reproductive age.
Rotation
Even a small degree of rotation distorts the mediastinal borders, and the lung nearest the film will appear less translucent. The following points should be stressed to obtain a true PA view (without rotation):
 PA view with rotation. Image courtesy of Dr. Naveed Ahmad.
PA view with rotation. Image courtesy of Dr. Naveed Ahmad.
- Ensure that the patient is standing evenly on both feet.
- Both shoulders should be rolled forward and downward.
- The chest radiograph should be well-centered so that the medial ends of the clavicle are equidistant from the vertebral spinous processes at T4/5. However, scoliosis and other thoracic deformities negate the value of conventional centering.
 PA view without rotation. Image courtesy of Dr. Naveed Ahmad.
PA view without rotation. Image courtesy of Dr. Naveed Ahmad.
Central ray
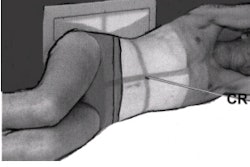
For PA, the chest landmark that is used for locating the center of the lung fields is the vertebra prominans (T1). It corresponds to the apical regions of both lungs. The vertebra prominans can be palpated at the base of the neck. The hand-spread method can be used to locate the central ray. To use this method, the technologist should know his or her own hand-spread width (most hands can reach 7 inches).
 Hand-spread method for central ray positioning utilizing the vertebra proinans. Image courtesy of Dr. Naveed Ahmad.
Hand-spread method for central ray positioning utilizing the vertebra proinans. Image courtesy of Dr. Naveed Ahmad.For the average adult, the central ray should be directed to the spinal column (mid-sagittal plane) approximately 7 inches (18 cm) for a female and 8 inches (20 cm) for a male down from the vertebra prominans. This corresponds to the level of T7 and the inferior angle of scapula, a source-to-image receptor (SID) distance of 72 inches (180 cm). Hypersthenic body types require only 7 inches down from the vertebra prominans, whereas athletic sthenic/hyposthenic types will require 9 inches down from the vertebra prominans.
Film holder (image receptor) placement
The horizontal dimension of an average chest is greater than the vertical dimension. This requires that a 14 x 17-inch film holder or image receptor (IR) be placed crosswise. However, depending on the body type, the most common practice is placing the film holder or IR lengthwise. Either lengthwise or crosswise, the goal is to adequately include the lateral lung margins.
Collimation
Collimation should be adequate to allow for some margin of error in central ray placement and lung expansion during deep inspiration. On each side of the posterior chest the illuminated field margins should correspond to the outer skin margins. The upper border of the illuminated field should be at the level of vertebra prominans (4 cm above the apex of lungs).This will result in a lower collimation border of 1-2 inches below the costophrenic angle, if the central ray was correctly centered.
Respiration
Be sure to make the exposure upon a second full inspiration by the patient. The patient should take as deep a breath as possible, and then hold it to fully aerate the lungs. Taking a second deep breath before holding it allows for a deeper inspiration, as more air is inhaled during the second breath than during the first breath.
 PA view on full inspiration. Image courtesy of Dr. Naveed Ahmad.
PA view on full inspiration. Image courtesy of Dr. Naveed Ahmad.
The best way to determine the degree of inspiration is to start at the top of the patient's rib cage, with rib number one, and count down to the tenth or eleventh rib posteriorly. A general rule for average adult patients is to show a minimum of 10 ribs on a good PA chest radiograph. Older patients have less inhalation capability, with a resulting low lung volume, which requires a higher central ray location.
Evaluation criteria for a good PA projection
- Entire lung fields from apices to costophrenic angles should be clearly demonstrated.
- No rotation. Rotation on a PA chest radiograph can be determined by examining both sternal ends of the clavicles for a symmetric appearance in relationship to the spine. On a true PA chest without any rotation, both the right and left sternal ends of the clavicle will be the same distance from the center line of the spine. The direction of rotation can be determined by which sternal end of the clavicle is closest to the spine.
- Trachea is visible in midline.
- Scapula projected outside the lung fields.
- Ten posterior ribs are visible above the diaphragm.
- There is a sharp outline of the heart and diaphragm.
- A faint shadow of the ribs and superior thoracic vertebrae is visible through the heart shadow.
- Lung markings are visible from the hilum to the periphery of the lung.
 Evaluation criteria for a good PA projection. Image courtesy of Dr. Naveed Ahmad.
Evaluation criteria for a good PA projection. Image courtesy of Dr. Naveed Ahmad.
Variations
An expiratory film may be helpful under some circumstances. A small pneumothorax (air in the pleural cavity) may be difficult to detect on a routine inspiratory PA film. On expiration, the volume of the thorax and lungs is reduced but the amount of air in the pleural space remains essentially unchanged. The pneumothorax then occupies a larger percentage of the area of the thorax and is more easily visible.
Another indication for an expiratory film is to demonstrate air trapping. The bronchi increase in diameter with inspiration, and decrease with expiration. With a foreign body or tumor in a main bronchus, a valve action may occur, with air bypassing the obstruction on inspiration and becoming trapped on expiration.
 Expiration PA view. Image courtesy of Dr. Naveed Ahmad.
Expiration PA view. Image courtesy of Dr. Naveed Ahmad.
With expiration, the normal lung is reduced in volume and becomes more radiopaque. The obstructed portion of the lung retains its air, thereby retaining its radiolucency and forcing the mediastinum to shift toward the contralateral side. If a patient has a unilateral respiratory wheeze, air trapping is likely, and an expiratory film may be helpful.
Imaging Technique
- Film size: 14 x 17 inches (35 x 43 cm) lengthwise or crosswise
- Exposure: 110 - 125 kVp range
- mAs: 3
- Sk: 17
- ML: 5
- cm: 22
- Focal Spot: small (large for obese patients)
- Bucky: yes (under the table)
- Film speed: 200
AuntMinnie.com contributing writer
October 19, 2001
Dr. Ahmad is a second-year resident affiliated with Columbia University's New York-Presbyterian Hospital. He is the owner and developer of RadQuiz.com, a compendium of radiology teaching files on the Internet.
Copyright © 2001 AuntMinnie.com