Despite its whiz-bang capabilities in imaging cancer patients, FDG-PET scans do have their pitfalls, particularly when it comes to nonmalignant chest abnormalities. In a pictorial essay in the American Journal of Roentgenology, Dr. Syed Asad and colleagues highlighted some of the infectious and inflammatory lesions that may mimic tumor.
The increase in FDG uptake can be attributed to the heightened metabolic state of accumulated inflammatory cells, wrote Asad who is from the department of neurology at Emory University Hospital in Atlanta. Asad’s co-authors are from the department of radiology at Massachusetts General Hospital in Boston.
A particularly common instance of this type of false positive occurs in pneumonia. "Pulmonary inflammation and pneumonia can manifest increased glycolysis and, as a result, FDG uptake," the authors explained (AJR, April 2004, Vol.182:4, pp.983-989).
Another lung disease to watch out for is sarcoidosis, a systemic granulomatous inflammatory disorder. The culprit in this instance is active inflammatory cells (multinucleated giant cells and lymphocytes, to name a couple), which will show FDG uptake.
 |
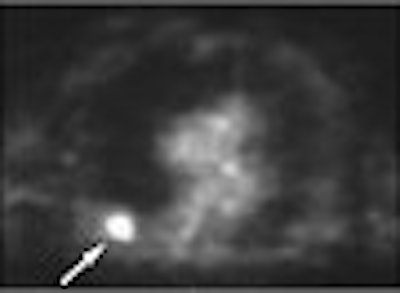
A 62-year-old man with a history of lung cancer and severe emphysema. CT scan (above) shows spiculated nodule (arrow) suggestive of either new primary tumor or recurrent disease. FDG-PET image (below) of thorax shows increased radiotracer uptake of FDG in nodule (arrow). Wedge resection was performed. Nodule was caused by atypical mycobacterial infection. Asad, S, Aquino SL, Piyavisetpat N, Fischman AJ, "False-positive FDG PET Uptake in Nonmalignant Chest Abnormalities," (AJR 2004 182; 983-989).
 |
In cases of pleural fibrosis, which can develop from asbestos exposure, "an important differential diagnosis for asbestos-related pleural disease is malignant pleural mesothelioma." In the authors' example, the FDG-PET scan was indicative of this serious illness. However, surgical biopsy confirmed benign inflammation, they said.
Finally, previous research has shown increased FDG uptake in the vasculature of patients at risk for atherosclerotic disease. But focal vascular uptake in the mediastinum may simulate metastatic lymph node disease. Anatomic clarification can be achieved with CT correlation.
The authors concluded that if imaging with either FDG-PET or CT cannot rule out neoplasia, then diagnostic biopsy would offer the definitive diagnosis.
These results support earlier reports on fine-tuning FDG-PET in thoracic imaging. Other disease processes or entities that can cause false-positives on mediastinal FDG-PET include caseating granulomas with active inflammation, Histoplasma organisms, and round atelectasis (Chest, October 1993, Vol.104:4, pp.997-1002; Journal of Computer Assisted Tomography, July-August 1998, Vol.22:4, pp.601-604).
A group from the Medical University of South Carolina in Charleston, SC, published a guideline for noninvasive imaging of non-small cell lung cancer (NSCLC). They wrote that FDG-PET has "proved useful in differentiating neoplastic from normal tissues" (Chest, January 2003, Vol.123:1 supplement, pp. 147S-156S).
But they cautioned that "the technique is not infallible as certain nonneoplastic processes,including granulomatous and other inflammatory diseases as well as infections, also may demonstrate positive PET imaging findings." The group also recommended that patients with abnormal FDG-PET findings may benefit from further evaluation of the mediastinum with sampling of the abnormal lymph node prior to surgical resection.
Another group from Emory University will present a paper on false-positive uptake on FDG-PET in granulomatous disease at the 2004 American Roentgen Ray Society meeting in Miami Beach, FL. On May 5, Dr. Matthew Hartman will discuss his group's experience with an integrated PET/CT protocol in pinpointing benign tumors.
By Shalmali PalAuntMinnie.com staff writer
April 9, 2004
Related Reading
MDCT pulmonary angiogram rules out PE for months, March 22, 2004
Chest x-ray benefits from CAD for spotting lung nodules, May 18, 2004
Chest CR outperforms screen-film catheter localization , May 26, 2003
MRI demonstrates fetal thymus, bronchial obstruction, May 12, 2003
Copyright © 2004 AuntMinnie.com

















