FDG-PET/CT scans are a valuable tool for staging women newly diagnosed with breast cancer, according to a study published online April 3 in Surgical Oncology. Researchers from Israel found a significant correlation between FDG uptake and breast tumor size and grade.
"PET/CT is highly useful in detecting axillary metastases, including cases with [ultrasound]-negative data and provides important information about the extent of axillary and extra-axillary lymph node involvement," said researchers led by Dr. Tima Davidson of Tel Aviv University.
The absence of distant metastases in women diagnosed with breast cancer is traditionally determined by a combination of several diagnostic tools such as bone scans, liver ultrasound, and CT of the chest and abdomen. During the last decade, however, PET/CT has become recognized as a tool for more precise diagnosis of distant metastases, as the intensity of FDG uptake can correlate with the aggressiveness of tumors.
In this study, researchers studied the role of PET/CT for evaluating axillary lymph nodes and distant metastases in patients with newly diagnosed primary breast cancer. They analyzed PET/CT reports of all breast cancer patients referred to Chaim Sheba Medical Center in Tel Hashomer between 2012 and 2017. Among patients with newly diagnosed primary breast cancer, the researchers looked at the association of FDG uptake with clinical variables of the primary tumor, including regional nodal status and the presence of distant metastases.
Out of 324 patients, they found 265 (81.8%) had focal uptake of FDG that corresponded with the cancerous lesion, and 21 (6.5%) had no FDG-avid findings. The remaining 38 patients had diffuse or nonspecific uptake of FDG. Among patients with a focal uptake of FDG, the mean tumor size was 2.6 cm ± 1.9 cm (range, 0.5-13.5 cm) and the mean SUVmax was 5.3 ± 4.9 (range, 1.2-25.0).
The researchers found that larger tumors tended to have higher FDG uptake as measured by SUVmax.
| Association of tumor size with SUVmax in FDG-avid breast cancer | ||
| Tumor size | Number of patients | Mean SUVmax |
| < 1.5 cm | 79 | 2.7 ± 2.4 |
| 1.6-1.9 cm | 46 | 4.3 ± 3.9 |
| 2.0-2.9 cm | 74 | 6.1 ± 4.6 |
| 3.0-5.0 cm | 45 | 7.4 ± 5.9 |
| 5.1 cm and more | 21 | 9.7 ± 6.7 |
| Total | 265 | 5.3 ± 4.9 |
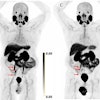
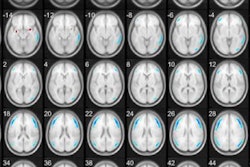
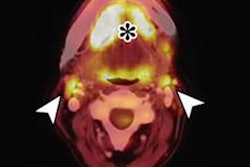
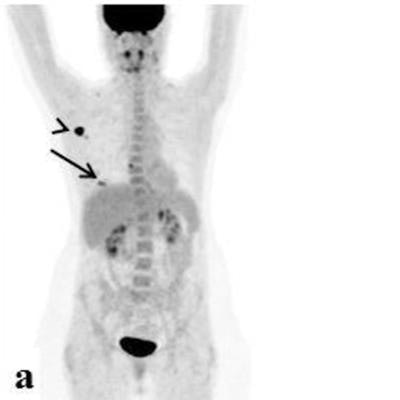
 FDG-avid multifocal breast lesions. An 84-year-old woman with a multifocal cancer in the left breast and multiple bone FDG-avid metastatic lesions. FDG-PET/CT: maximum intensity projection (MIP) (a), a representative PET (b), and CT axial slices (c). Image courtesy of Surgical Oncology.
FDG-avid multifocal breast lesions. An 84-year-old woman with a multifocal cancer in the left breast and multiple bone FDG-avid metastatic lesions. FDG-PET/CT: maximum intensity projection (MIP) (a), a representative PET (b), and CT axial slices (c). Image courtesy of Surgical Oncology.In addition, distant FDG-avid lesions were detected in 33 patients (10.2%). Seven patients without distant metastases had FDG-avid supraclavicular lymph node involvement and four had FDG-avid internal mammary lymph nodes.
Forty-five (13.9%) out of the 324 patients had unexpected findings on FDG PET/CT studies. These cases resulted in changes in the treatment approach selected prior to the PET/CT. An additional 21 patients with FDG-avid level 2-3 axillary lymph nodes needed modifications to their original surgical or radiation plans.
"Overall, disease management changed for 66/324 patients (20.4%) following PET/CT studies," the authors noted.
Despite growing data about the usefulness of PET-CT in breast cancer staging, current guidelines do not support routine use of this diagnostic tool, the researchers wrote. One of the arguments against the use of PET/CT for breast cancer staging is the increasing proportions of overdiagnosed, indolent, and nonaggressive tumors that have been detected.
In this study, while 82% of newly diagnosed breast cancer patients had localized pathological FDG uptake that corresponded with a cancerous lesion, 6.5% of patients with known breast cancer did not have an FDG-avid finding. Low FDG uptake was associated with grade-I tumors, lobular histology, and a small primary tumor size. Such conditions do not justify the use of PET/CT for breast cancer staging, the researchers said.
"Generally, PET/CT is a useful diagnostic tool for staging breast cancer patients, but indications for its use should be limited to specific clinical situations," they concluded.