SAN DIEGO - FDG-PET is a considerably better predictor of treatment response and outcome than fluoride-PET for breast cancer patients with metastatic bone lesions, concluded researchers on Tuesday at the Society of Nuclear Medicine and Molecular Imaging (SNMMI) conference.
A group from the University of Washington found that FDG-PET was better able to forecast time to progression, skeletal-related events, and overall survival, while fluoride-PET did not provide enough information to predict any response in women who received both types of scans.
"Fluoride-PET is very good at staging, but we did not find it predictive at all for response to therapy, whereas we did find that changes in FDG between scans were predictive of response to therapy," lead author Lanell Peterson, a research scientist at the Seattle Cancer Care Alliance, told AuntMinnie.com.
Detection challenges
Bone is the most common site of breast cancer metastases, occurring in up to 80% of breast cancer patients, Peterson told SNMMI attendees.
 Lanell Peterson from the Seattle Cancer Care Alliance.
Lanell Peterson from the Seattle Cancer Care Alliance."These lesions are often difficult to assess for response by conventional imaging such as CT and bone scans," she said. "We have also seen that fluoride-PET can improve bone metastases detection when compared to bone scans, and prior retrospective work in our group has shown that FDG-PET helped predict time to progression and risk of skeletal-related events."
So, for this study, Peterson and colleagues sought to evaluate fluoride- and FDG-PET prospectively to assess response to therapy and risk of skeletal-related events in patients starting a new therapy for their bone-dominated breast cancer. The study analyzed 24 patients between 2004 and 2012 (mean age, 56 years; range: 33-91 years) who completed fluoride-PET and FDG-PET scans prior to treatment and again approximately four months after the start of therapy.
The four-month follow-up scans were timed to coincide with patients beginning their next round of therapy. The majority of patients (65%) had primary ductal cancers. Approximately one-third were treated with chemotherapy, with 16 women also having hormonal therapy and eight receiving radiation treatment. The average number of therapies prior to tumor removal was 2.4.
Fluoride- and FDG-PET images were taken from the base of the skull to the midthigh. Maximum standardized uptake values (SUVmax) were calculated for as many as five lesions, with index lesions identified as having the highest SUVmax for both fluoride and FDG. Time to progression and skeletal-related events were determined by clinical follow-up. Overall survival was the time from a patient's first fluoride-PET scan to the date of death.
At a median time of 37 months for clinical follow-up, 23 patients (88%) had died from cancer, with a median overall survival of 1,130 days (3.1 years). Twenty-four women (92%) had confirmed disease progression (median time to progression, 186 days), while 16 (62%) had skeletal-related events (median time to skeletal-related events, 981 days).
Predicting treatment response
In the univariate analysis, which included SUVs of the index lesions for each fluoride and FDG scan or the percentage difference between the scans, neither initial nor follow-up fluoride or FDG data were able to predict a patient's time to disease progression, a skeletal-related event, or overall survival.
However, the multivariable analysis, which included the FDG SUVmax of the first scan, the percentage change between baseline and follow-up PET imaging, and a patient's elevated tumor markers when she entered the study, showed more significant findings.
For example, a 35% reduction in FDG SUVmax from the baseline to the follow-up scan was associated with a 60% reduction in the risk of disease progression and a 40% reduction in the risk of death. Conversely, an increase of 6.3 SUV units was associated with an 18% increase in the risk of disease progression, a 40% increase in the risk of a skeletal-related event, and a 20% increase in the risk of death.
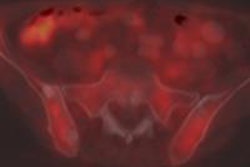
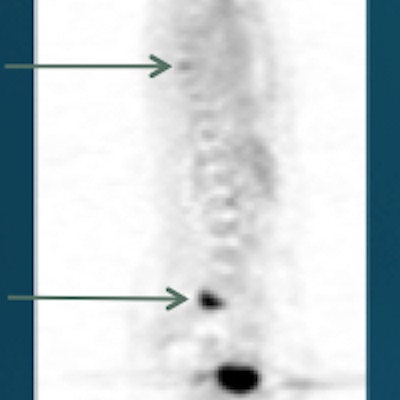
 A 49-year-old woman with a first recurrence of breast cancer at time of the study 12 years after primary treatment. FDG decreased somewhat between scans, while fluoride-PET showed both increased and decreased SUVs. The patient was treated with letrozole (plus Herceptin) and switched to Faslodex after these scans. She eventually died of her disease seven years later. Image courtesy of Lanell Peterson.
A 49-year-old woman with a first recurrence of breast cancer at time of the study 12 years after primary treatment. FDG decreased somewhat between scans, while fluoride-PET showed both increased and decreased SUVs. The patient was treated with letrozole (plus Herceptin) and switched to Faslodex after these scans. She eventually died of her disease seven years later. Image courtesy of Lanell Peterson."Based on this prospective data, we found that fluoride was not predictive of any clinical end point," Peterson said. "And, if FDG SUVmax is high prior to the start of therapy or remains high [through the second scan], then there is an increased risk of progression, skeletal-related event, or death."
In light of the results, Peterson and colleagues affirmed FDG-PET's role in assessing response to therapy in women with bone-dominant breast cancer, as well as its role in future clinical trials.
"Based on our previous studies, we weren't surprised that FDG did well," Peterson told AuntMinnie.com. "I don't think we were completely surprised that fluoride did not do particularly well. Fluoride-PET is still useful for initial evaluation when a patient is suspected of cancer and may have bone metastases, and it may be better than bone scans, especially those that are osteoblastic."