Bone health agents should be mandatory to help prevent fractures in men who receive radionuclide therapy with radium-223 for prostate cancer, according to a study published online April 4 in Clinical Genitourinary Cancer.
It was already known that radium-223 for the treatment of metastatic castration-resistant prostate cancer (mCRPC) increases the risk of fracture when used in combination with abiraterone and prednisolone. However, the effect of radium-223 monotherapy on fracture risk has not been well documented, according to researchers.
"Our data suggests that radium-223 may also increase the risk of fracture when used as a single agent," said Dr. Chris Parker of the Royal Marsden Hospital in the U.K.
Radium-223 is a bone-seeking alpha-emitting radionuclide used in mCRPC. The risk of fracture in men receiving radium-223 monotherapy is unclear; one hypothesis is that radium-223 increases the risk of fracture only if used in combination with other agents that have an adverse effect on bone health, such as abiraterone and prednisolone.
In this prospective study, researchers looked at the incidence of fracture in 36 men treated with radium-223 compared with a cohort of 36 patients who were not treated with the radionuclide. Patients with chemotherapy-naive, bone-only, progressive mCRPC were enrolled. They received treatment with radium-223 every four weeks for up to six cycles.
Patients were randomized to one of two dose levels with radium-223, 55 or 88 kBq/kg. To assess fractures, whole-body MRI scans were done at baseline, at cycle 2 and 4, and at one month post-treatment. During the follow-up period, patients were evaluated every four months for one year, following which, imaging was done according to routine clinical practice and scans were collected and reviewed centrally.
In total, 205 imaging scans in patients after they started radium-223 treatment were evaluated. Overall, 74 new fractures were identified in 20 (56%) patients on the MRI scans. Freedom from fracture was 79% at six months and 56% at 12 months, while the median time to first new fracture was 13.6 months.
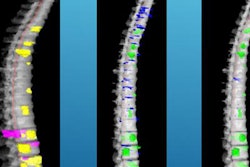
 Sagittal T2-weighted MRI spine images in a 71-year-old man with mCRPC, at baseline (a), and two years after six cycles of radium-223 (b). Follow-up images show multiple nonmalignant endplate vertebral fractures at T7, T8, T9, T10, T12, and L4 (white arrows) with significant vertebral collapse at T10 and T12. Images courtesy of Clinical Genitourinary Cancer and Dr. Chris Parker, et al. Licensed under CC BY-NC-ND 4.0.
Sagittal T2-weighted MRI spine images in a 71-year-old man with mCRPC, at baseline (a), and two years after six cycles of radium-223 (b). Follow-up images show multiple nonmalignant endplate vertebral fractures at T7, T8, T9, T10, T12, and L4 (white arrows) with significant vertebral collapse at T10 and T12. Images courtesy of Clinical Genitourinary Cancer and Dr. Chris Parker, et al. Licensed under CC BY-NC-ND 4.0.Most new fractures developed within the axial skeleton. Out of all fractures, 50 occurred at a site of uninvolved bone. Of the 20 patients who had new fractures, 10 had symptomatic fractures, four had asymptomatic fractures, and six had uncertain symptomatic status.
| Fracture location and distribution based on bone status | |||
| Fracture location | Patients (%) | New fractures | New fractures at site of metastasis |
| Spine | 14 (38.9%) | 49 | 15 |
| Thorax | 7 (19.4%) | 19 | 4 |
| Pelvis | 4 (11.1%) | 5 | 4 |
| Extremities | 1 (2.8%) | 1 | 1 |
| Total | 20 (55.6%) | 74 | 24 |
The researchers found that 44% of men with metastatic castration-resistant prostate cancer treated with radium-223 as a single agent had new fractures at one-year follow-up, and most of the fractures were of uninvolved bone and not at the site of metastases. This indicates that men receiving the treatment are at high risk of fracture and should be given bone health agents to prevent fracture, the authors noted.
"Our policy is to recommend the use of an oral bisphosphonate, such as alendronic acid, in men starting long-term androgen deprivation," they concluded.