Approximately 60,000 lower limb amputations are performed annually in the U.S., and many of these patients experience residual pain ranging from postoperative complications to phantom pain. But when clinical manifestations are nonspecific, diagnosing the various causes of stump pain can be difficult. Imaging, including x-ray and MRI, can help determine the causes of this pain and limit the psychological and socioeconomic difficulties associated with amputation, according to French investigators.
In the latest issue of RadioGraphics, Dr. Philippe Henrot and his co-authors from the Central University Hospital of Nancy in Vandoeuvre-les-Nancy offer a comprehensive guide to imaging both amputees with prostheses and those without who are experiencing stump pain.
"Very little data regarding imaging for stump pain has been published in the radiology literature, and most of these data deal with neuroma. However, radiologic evaluation has proved to be helpful in many cases in conjunction with physical exam," the authors wrote (RadioGraphics, October-November 2000, Vol.20, pp.219-235).
The causes of stump pain are divided into two groups: Pain that is brought on by the presence of a prosthesis and non-prosthesis-induced pain, such as heterotopic ossification.
To diagnose heterotopic ossification frequently encountered at the stump end, Henrot and colleagues recommend conventional radiography with anteroposterior and lateral weight-bearing views. However, soft-tissue damage with inflammatory changes is seen better with T1-weighted axial and coronal MRI.
"Conventional radiography is the easiest modality to depict all the pathologic processes of osseous origin," Henrot told AuntMinnie.com. "It can recognize not only a heterotopic ossification, but also an aggressive bone edge, inappropriate length of the stump, a tumor recurrence, or osteomyelitis. In the case of indeterminate origin of pain after x-ray, the next imaging step is decided jointly [by the radiologists and referring physicians], and most of the time it’s MRI."
The group also preferred MRI for detecting cancer and tumor recurrence. Local tumor recurrence may occur many years after amputation for neoplasm because of microscopic skip metastases or the implantation of the tumor cells in the soft tissue at the time of surgery, they wrote.
"Imaging protocol for MR detection of local recurrence does not differ from other indications. It’s essential to perform T1 sequences to analyze medullar bone and fat planes. T2 sequences can depict inflammation and ancillary diagnoses, i.e. bursitis. T1 sequences in two orthogonal planes with gadolinium and fat saturation are indicated to depict enhancement of the tumor, and even skip metastases," he said.
While Henrot recommended periodic imaging evaluation to catch recurrence, screening these patients on a regular basis may not be worthwhile.
"In our experience with 35 amputee patients, tumor recurrence of the stump is uncommon. The one patient we had with an amputation for cancer had no abnormality in his stump on MRI, but a metastatic lung disease," he explained.
Perhaps the most challenging source of stump pain for clinicians and radiologists is phantom pain, a pathologic condition that develops following amputation that is described as a "burning or crushing sensation or paresthesia." The evolution of this condition varies depending on physical energy level and mood. The primary purpose of imaging is to exclude neuroma, which may simulate phantom limb pain, the paper states.
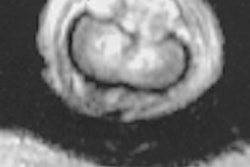
"Phantom pain associated with a mass at physical exam or a Tinel’s sign [distal tingling on percussion] should require an MRI to depict neuroma," Henrot said. The image above shows a sciatic neuroma.
Neuroma is a non-neoplastic proliferation that occurs at the end of an injured nerve and is generally seen one month to one year after amputation. Neuroma has low signal intensity on T1-weighted images and intermediate to high signal intensity on T2-weighted images. It also demonstrates variable enhancement after administration of gadopentetate dimeglumine.
Other issues addressed by the group include bursitis and soft-tissue inflammation, stress fracture, and other prosthesis-induced stump pain.
By Shalmali PalAuntMinnie.com staff writer
December 20, 2000
Click here to post your comments about this story. Please include the headline of the article in your message.
Copyright © 2000 AuntMinnie.com