Indoor volleyball has never been as sexy as its beach-based cousin, but for years it had a quadrennial moment in the Olympic sun all to itself. Since the 1996 Olympics in Atlanta, though, the hard courts have had to share the glory with sand courts, while still doling out a greater share of the sport's injuries.
Beach volleyball can claim exclusively perhaps two injuries: sunburn and "sand toe" -- a hyperplantarflexion or knuckling over of the toe caused when a toe of a barefoot player is caught in the sand (FootCareMD.com).
Besides that, beach volleyball is easier on the body than the indoor game. The court is smaller so players put less stress on their shoulders. The sand surface is also much more forgiving than a gym floor, resulting in fewer overuse injuries such as patellar tendinopathy (jumper's knee) and acute injuries, including ankle sprains and torn menisci (The Physician and Sportsmedicine, March 1999, Vol. 27:3).
Visualization of the meniscus has long been the domain of MRI, of course. Yet, a new study in the American Journal of Roentgenology is the first to assess the value of standard axial images for meniscal tears, both alone and in conjunction with coronal and sagittal images, which already have proved valuable in this area (AJR, July 2004, Vol. 183:1, pp. 9-15).
Researchers at the University of California, San Diego examined 62 patients with a 1.5-tesla scanner using a dedicated knee coil. Imaging sequences included axial fat-saturated fast spin-echo proton density (TR range/TE range, 2,650-2,717/12-54), coronal fat-saturated fast spin-echo proton density (3,000-3,400/15-65), and sagittal spin-echo proton density (TR range/TE, 2,117-2,367/30). The sequences were obtained with a 4-mm slice thickness in 43 patients and a 5-mm slice thickness in 19 patients.
The images for each patient were analyzed for accuracy along the three individual planes and in two-plane combinations. All findings were confirmed by arthroscopy.
 |
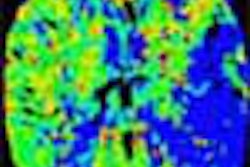
| Sixty-six-year-old man with radial tear of lateral meniscus. Above, axial fat-saturated fast spin-echo proton density-weighted image (TR/TE, 2,717/54; slice thickness, 4 mm) of right knee shows well-defined linear increased intensity (arrow) in body of lateral meniscus starting from free edge. Below, coronal fat-saturated fast spin-echo proton density-weighted image (3,750/60; slice thickness, 4 mm) shows tear as vertical defect in body of lateral meniscus (arrow). Tarhan NC, et al, "Meniscal Tears: Role of Axial MRI Alone and in Combination with Other Imaging Planes," (AJR 2004, Vol. 183, pp. 9-15). |
 |
The most dramatic impact of axial imaging was the reduction of false-positives. Among 16 patients with no meniscal tearing, axial imaging was the only method to correctly diagnose every patient. The authors also found no significant difference in accuracy between the axial plane and other imaging groups, and postulated that axial images are just as useful in diagnosis.
Axial slices were especially useful in diagnosing the lateral meniscus. Of the 16 correct "no-tear" assessments, 14 were made on the lateral side. The authors promised to conduct further study, based on the particular success of the axial plane, in diagnosing radial or complex tears of the posterior horn.
The radial tear, running perpendicular to the long circumferential axis of the meniscus, is considered a difficult injury to see on MRI. And a new study from the Neuroimaging Institute in Melbourne, FL, claims that the standard menisectomy may actually cause radial tears in up to 50% of patients (AJR, April 2004, Vol. 182:4, pp. 931-936).
 |
| Twenty-eight-year-old man with knee pain after surgery. Patient had surgically proven meniscal radial tear. Above, proton density-weighted sagittal MR image (TR/TE, 1,800/12) shows findings consistent with meniscal radial tear (arrow). Below, T2-weighted sagittal MR image (3,950/51) shows linear radial tear (arrow). Magee T, Shapiro M, Williams D, "Prevalence of Meniscal Radial Tears of the Knee Revealed by MRI After Surgery," (AJR 2004, Vol. 182, pp. 931-936). |
 |
"Meniscal resection may alter the hoop mechanism of the meniscus, and decrease the ability of the meniscus to transmit loads," the authors wrote. "This circumstance may predispose the remaining intact meniscus to injury, and specifically place the meniscus at risk for radial tears because of the altered hoop mechanism of the knee."
In this prospective study, 100 patients who underwent menisectomy were re-examined with MRI. Forty-two of the patients underwent an additional MR arthrography, in part because postoperative tears are difficult to see on MRI. None of the available operative reports on 92 of the patients mentioned a radial tear.
The prevalence of radial tearing in postoperative knees was 32%, compared to a reported 14% in untreated knees. Twenty-six of the tears were in the lateral meniscus.
For visualizing the radial tears, the authors recommended using T2-weighted fast low-angle axial images, with T1 coronal and sagittal images, and T2 proton density fat-saturated sagittal images. And to cope with the added challenges of postoperative imaging, they also advised looking for oblique evidence of radial tearing: meniscal truncation, abnormal morphology, lack of continuity, and linear areas of abnormal increased signal on T2-weighted images.
By Matt King
AuntMinnie.com contributing writer
August 28, 2004
Related Reading
Tunnel-view x-ray holds the key to locked-knee syndrome, March 12, 2004
MRI pinpoints meniscal tears, proves less valuable for knee trauma, January 9, 2003
MR arthrography not always needed in post-operative knees, February 13, 2002
Copyright © 2004 AuntMinnie.com