Combining diffusion-weighted MRI (DWI-MRI) with dynamic contrast-enhanced MRI to calculate apparent diffusion coefficient (ADC) values could decrease false-positive findings in breast MRI and reduce preventable biopsies, according to a new study published online on October 2 in Radiology.
Researchers from the University of Washington School of Medicine and Seattle Cancer Care Alliance also found that DWI's ability to differentiate between high-risk lesions and other nonmalignant tumor subtypes could enhance patient care and treatment management.
DWI measures ADC values, which relate to the movement of water molecules in vivo and indirectly reflect tissue microstructural characteristics. Hence, as lead study author Dr. Sana Parsian and colleagues noted, DWI has been used primarily in neurological applications (Radiology, October 2, 2012).
However, more recently, DWI has been used with increasing frequency for breast imaging because it can help distinguish between benign and malignant breast lesions. DWI has also shown that low ADCs for breast carcinomas can indicate normal tissue or benign lesions.
In this study, researchers retrospectively reviewed an MRI database to identify consecutive suspicious breast lesions detected by MRI from October 2005 to December 2008 that subsequently were sampled with a core needle or surgical biopsy.
A total of 175 nonmalignant lesions from 162 examinations among 161 women (median age, 48 years; range, 27-77) were included in the analysis. Lesions were assigned a BI-RADS assessment of 4 for suspicion of malignancy or 5 for a great suspicion of malignancy.
Cancer diagnoses
The MRI exams initially were conducted for various clinical indications: to evaluate the extent of disease in patients with newly diagnosed breast cancer in 83 (51%) of 162 studies, high-risk screening in 64 (40%), the need for additional study in 12 (7%), and short-term follow-up in three (2%).
All MRI scans were performed on a 1.5-tesla system (Signa LX, GE Healthcare) using a dedicated eight-channel bilateral breast coil. DWI was performed after the dynamic contrast-enhanced imaging acquisition by using a DWI echo-planar imaging sequence with parallel imaging and fat suppression.
The researchers also compared ADC values for the 175 lesions with those of normal fibroglandular tissue in each patient. In addition, the mean ADC values of benign and high-risk subtypes were compared with malignant lesions in a previous study, which included 15 invasive ductal carcinomas, five invasive lobular carcinomas, and 11 cases of ductal carcinoma in situ.
The most common histologic subtype was fibroadenoma, at 30, followed by 23 subjects with atypical ductal hyperplasia (ADH), 21 with adenosis, and 19 with focal fibrosis. Four lymph nodes included in the study were described as suspicious masses at MRI and subsequent ultrasound.
 |
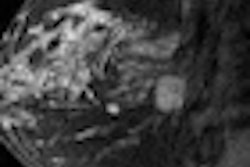
| Images are of a 61-year-old woman with a history of right-breast ductal carcinoma in situ. Axial dynamic contrast-enhanced MRI image (above) shows 13-mm lobular heterogeneously enhancing mass (arrow) in the subareolar region of the left breast. All images courtesy of Radiology. |
 |
| The lesion (arrow) is hyperintense on axial DWI (above) and has a low ADC on an ADC map (below). No evidence of carcinoma was detected at excisional biopsy. |
 |
Maximum lesion size, as defined with dynamic contrast-enhanced MRI, ranged from 0.2 to 9.1 cm, with a median size of 1.1 cm. Lesion types included 92 (53%) masses, 78 (45%) areas of nonmasslike enhancement, and five (3%) foci. A total of 28 (16%) lesions were high-risk lesions (ADH or lobular neoplasia).
Of the 175 benign and high-risk false-positive lesions found with dynamic contrast-enhanced MRI, 81 (46%) foci with positive lesions had ADCs above the diagnostic threshold. The most common lesion subtypes with ADCs above the threshold were fibroadenoma (19 of 30 cases, or 63%), adenosis (11 of 21 cases, or 52%), and focal fibrosis (10 of 19 cases, or 53%). That total comprised approximately half of the lesions with ADCs above the threshold.
By comparison, the most common lesion subtypes with ADCs below the threshold were ADH (18 of 23 cases, or 78%), fibroadenoma (11 of 30 cases, or 37%), and adenosis (10 of 21 cases, or 48%). These accounted for approximately 41% of lesions with ADCs below the threshold.
The key finding of the study is that DWI helped successfully characterize 46% of nonmalignant breast lesions assessed as false-positive findings by dynamic contrast-enhanced MRI as benign on the basis of ADCs above the study's diagnostic threshold, according to Parsian and colleagues.
In addition, among the most common false-positive lesion types, high-risk lesions, such as ADH and lobular neoplasia, "exhibited significantly lower mean ADCs than benign lesions and accounted for the most common false-positive MRI finding after implementing the ADC threshold," the authors wrote.
As for the next step, the researchers plan to conduct a multicenter trial to validate the findings and determine how to best incorporate ADCs into clinical breast MRI interpretations.