![]()
At the American Association of Physicists in Medicine (AAPM) annual meeting held in July in Philadelphia, researchers presented strategies for reducing dose while retaining imaging information.
This target of reducing the imaging dose without sacrificing tumor localization accuracy was addressed by Dan Ruan, PhD, an instructor in radiation oncology and radiation physics at Stanford University School of Medicine in Stanford, CA. "The basic idea is to introduce the Image Gently rationale into image-guided radiotherapy," she explained.
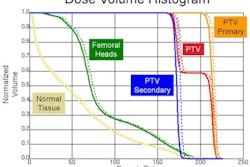
Typically, image-guided radiation therapy (IGRT) involves recording x-ray images at a fixed temporal rate during treatment to validate the tumor location and subsequently adjust treatment. Increasing the imaging frequency improves the localization accuracy -- but ups the dose to the patient. Ruan described a novel adaptive imaging protocol that aims to improve localization accuracy by imaging "smarter," rather than more often.
The idea is to fully utilize nonionizing-based observations, but to only trigger x-ray imaging when necessary. In a pilot study, Ruan and colleagues developed a mathematical model using an oracle controller, which identifies inconsistent events as the motion progresses (with respect to a given predictive presentation) and triggers x-ray imaging sparingly at those moments. This oracle triggering strategy distributes the imaging events nonuniformly in time, so as to maximize localization accuracy over the treatment.
The researchers performed a feasibility study on 159 patient-derived abdominal and thoracic tumor traces. "Our goal was to establish the performance upper bound between imaging dose and localization accuracy, and to determine the potential to reduce dose via adaptivity," Ruan explained.
Comparing oracle-triggered adaptive sampling with fixed-rate sampling revealed that for the same localization accuracy, adaptive imaging decreased the number of imaging events by 40% to 50%, effectively halving the dose delivered to the patient. Conversely, for the same imaging dose, adaptive imaging reduced localization errors by about 50%.
"We have demonstrated the potential for more gentle IGRT with adaptive imaging," Ruan concluded. "Of course, the performance depends on the representation used in the prediction. We are currently developing working heuristics based on the oracle insight and integrating this scheme into a prototype system at Stanford."
Grid benefits
Researchers at Henry Ford Health System in Detroit, meanwhile, have developed a scheme that reduces patient dose and improves image quality -- in terms of reducing scatter artifacts and enhancing the contrast-to-noise ratio -- in conebeam CT (CBCT) for IGRT.
"CBCT has advantages over 2D imaging in IGRT because it provides 3D visualization and offers the potential for adaptive radiotherapy," Jian-Yue Jin, PhD, a physicist in the department of radiation oncology, explained to the AAPM meeting delegates. "However, it delivers a high imaging dose and degraded image quality due to scatter."
Scatter artifacts can be reduced via direct scatter reduction methods or postscan compensation. Jin and colleagues have combined the two approaches, using a one-dimensional lead grid placed between the x-ray source and the patient during CBCT acquisition. The grid physically reduces scatter by blocking half of the beams, while recording partial image data from the unblocked regions. Simultaneously, scatter can be measured from the blocked regions beneath the grid, enabling postscan scatter correction.
The researchers evaluated this approach using phantoms and a Trilogy CBCT system (Varian Medical Systems, Palo Alto, CA) in single-rotation mode. They used interpolation to fill in the missing data in the partially blocked projections and reconstruct full CBCT images. The resulting images exhibited reduced scatter-related artifacts and improved contrast-to-noise ratio, in comparison to conventional CBCT, making them suitable for use in IGRT.
The single-shot mode reduces imaging dose by a factor of two, compared to conventional CBCT, with a trade-off of a reduction in longitudinal resolution, although the researchers found that this will not compromise 3D visualization and target localization accuracy. The dose is further reduced by employing a limited number of projections along with a total variation-based reconstruction algorithm. "The combination of single-shot mode and limited projections can reduce the total dose by a factor of 12," Jin said.
By Tami Freeman
Medicalphysicsweb editor
September 10, 2010
Related Reading
Conebeam reconstruction method speeds processing, cuts dose, July 21, 2010
ASTRO, ACR publish joint guidelines for radiation therapy, January 29, 2010
Adaptive radiation therapy monitors tumor change, December 25, 2009
© IOP Publishing Limited. Republished with permission from medicalphysicsweb, a community Web site covering fundamental research and emerging technologies in medical imaging and radiation therapy.





_p888_f1_thumb.png?auto=format%2Ccompress&fit=crop&h=167&q=70&w=250)










