Ultrasound can help predict ovarian cancer in women by classifying adnexal lesions via classic- or nonclassic-appearing imaging features, according to research published March 22 in Radiology.
Along with high sensitivity and specificity, a team led by Dr. Akshya Gupta from the University of Rochester Medical Center in New York also found that isolated nonclassic lesions with blood flow saw the highest cancer risk in women over the age of 60.
"This classic-versus-nonclassic approach to isolated adnexal lesions could be helpful to radiologists in a busy clinical practice so that they can more quickly assess a lesion and recommend management," Gupta and colleagues wrote.
Ultrasound is the first line of imaging for examining abnormalities in the pelvic area, including lesions that could indicate ovarian cancer. Classic lesions are commonly detected by ultrasound. These include benign simple cysts, hemorrhagic cysts, endometriomas, and mature cystic teratomas.
Nonclassic lesions, meanwhile, include lesions with a solid component and blood flow detected on Doppler ultrasound. These include multilocular cysts, cysts with solid components, and mostly solid lesions.
It's a challenge for radiologists to assess cancer risk when an adnexal lesion does not fit into one of the classic-appearing lesion categories. This also goes for when metastatic disease isn't present. Radiologists identify specific lesion features that would influence decision-making between surgery and additional imaging.
Risk stratification systems can be employed, but they can be difficult and time-consuming for radiologists to learn and use, researchers said.
Gupta et al wanted to test the performance of a strategy based on ultrasound classification for triaging women at average risk of ovarian cancer without compromising diagnostic performance. They also wanted to find out how well age or imaging features can predict cancer risk, using classic and nonclassic features.
The team gathered data from 878 women with a total of 970 isolated adnexal lesions in their retrospective study.
They found that their classification strategy had a sensitivity of 92.5% (49 of 53 lesions) and a specificity of 73.1% (669 of 917 lesions) for detecting malignancies.
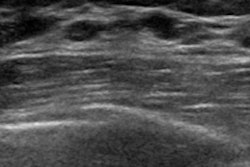
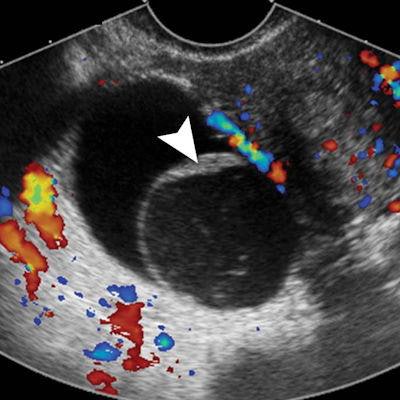
 A multi-institutional research team found that pelvic ultrasound can be a good predictor of whether adnexal lesions will become ovarian cancer. (A) Transverse color Doppler image of right adnexa shows what's consistent with a nonclassic lesion without blood flow. This multilocular cystic lesion shows smooth septation and no Doppler flow. (B) Transverse color Doppler image of right adnexa is compatible with a nonclassic lesion with blood flow. It shows a multilocular cystic lesion with solid component and internal Doppler flow. Image courtesy of RSNA.
A multi-institutional research team found that pelvic ultrasound can be a good predictor of whether adnexal lesions will become ovarian cancer. (A) Transverse color Doppler image of right adnexa shows what's consistent with a nonclassic lesion without blood flow. This multilocular cystic lesion shows smooth septation and no Doppler flow. (B) Transverse color Doppler image of right adnexa is compatible with a nonclassic lesion with blood flow. It shows a multilocular cystic lesion with solid component and internal Doppler flow. Image courtesy of RSNA.Women with average risk for ovarian cancer had a 1% frequency of malignancy in lesions with classic ultrasound features showing simple cysts, hemorrhagic cysts, endometriomas, or dermoids. Lesions that had a solid component with blood flow had a 32% (33 of 103) frequency of malignancy. This was higher in women older than 60, with a frequency of 50% (10 of 20).
The study authors wrote that their results had similar high sensitivity, specificity, positive predictive value, and negative predictive value for malignancy compared with other published algorithmic risk stratification systems. This includes a higher positive predictive value for detecting cancer when lesion blood flow and patient age were factored in.
They suggested that patients can be reassured that their lesion is benign when classic benign features are seen. Additional imaging can be considered if a nonclassic lesion with no blood view is seen, they added.
"In women with a nonclassic lesion with blood flow, particularly older women, referral to a gynecologic oncologic surgeon will help ensure expeditious treatment of possible ovarian cancer," they wrote.
In an accompanying editorial, Dr. Deborah Baumgarten from the Mayo Clinic in Jacksonville, FL, wrote that simplifying radiologists' approach to characterize adnexal lesions into classic and nonclassic categories "may be enough."
"We trust our gut that when something seems amiss, we look again and perhaps recommend a close follow-up," Baumgarten wrote. "We try to be consistent, and if there are competing guidelines, it's okay to choose the one that we will be more likely to use."