Lobular carcinoma in situ (LCIS) is a relatively rare high risk marker for breast cancer, but LCIS lesions found on core needle biopsy should be removed, according to a new study published in the February issue of the American Journal of Roentgenology.
As breast imaging technology has advanced, breast imagers are detecting subtle calcifications and masses more frequently. This is good news, but there is still little agreement among clinicians on how to handle some of these more subtle findings.
One aspect particularly in dispute is how to handle LCIS found at needle biopsy. Patient management options range from close imaging surveillance or open surgical biopsy to prophylactic chemotherapy or mastectomy, according to lead author Dr. Stamatia Destounis from Elizabeth Wende Breast Care.
Destounis and colleagues opt in favor of surgical excision after diagnosis based on core needle biopsy in the current study, which attempts to clarify confusion over how to manage these cancers (AJR, February 2012, Vol. 198:2, pp. 281-287).
An LCIS diagnosis implies that a patient has a 15% chance of developing an invasive cancer in the same breast or in the contralateral breast over the subsequent 30 years, the team wrote. The condition is rare but has been diagnosed increasingly since the 1980s: The current incidence rate of LCIS is 0.5% to 3.6% of core biopsies.
However, with no way of predicting who will have invasive disease, guidelines should be in place when a diagnosis of LCIS is made at core needle biopsy, Destounis and colleagues wrote.
"The radiologist's role when advising patients after a diagnosis of LCIS should be clear, but as [previous reports] show, inconsistency exists, which is why studies to date continue to waver between imaging follow-up and open surgical biopsy," they wrote.
The study included 64 diagnoses of LCIS in 60 patients ranging in age from 36 to 93 years. The lesions included:
- 39 calcifications
- 2 masses with calcium
- 10 masses
- 2 asymmetries
- 2 architectural distortions
- 2 architectural distortions with calcifications
- 7 MRI enhancements
Mammography detected lesions in 84% of the cases, missing 16%. Sonography detected lesions in 30% of the cases, missing 70%. Core needle biopsy was performed in all cases; there were 49 stereotactic biopsies, 12 ultrasound-guided biopsies, and three MRI-guided biopsies.
All but one case proceeded to surgery, the team wrote. Open surgical biopsy revealed 21 cancers (33%); of the remaining cases, 53% were atypical or high risk and 14% were benign.
 |
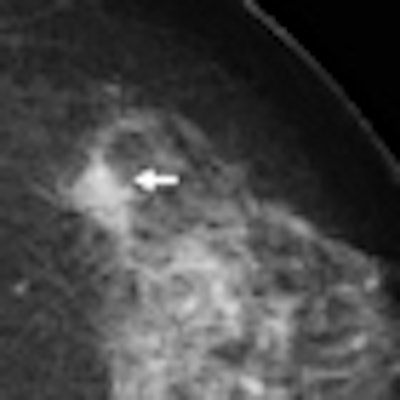
| 65-year-old woman who presented for routine screening mammography. Mammographic craniocaudal (left) and mediolateral oblique (right) views show irregular mass (arrow) with pleomorphic calcifications in left 1:30 area. All images courtesy of the American Roentgen Ray Society. |
 |
| Magnification view shows mass (arrow) with irregular microcalcifications. |
 |
| Ultrasound image (left) reveals subtle, hypoechoic, ovoid-shaped, 2-cm mass (arrow) containing numerous echogenic foci. Ultrasound-guided needle core biopsy image (right) reveals LCIS. At open surgical biopsy, diagnosis of infiltrating lobular carcinoma was made. |
"The results of our small study show that radiographic findings were present in a majority of histopathologically confirmed cases of LCIS at needle core biopsy," the team concluded. "[And since] cancer was diagnosed in our study in 33% of the cases at open surgical biopsy ... open surgical biopsy should be recommended after a core diagnosis of LCIS."