Digital breast tomosynthesis (DBT) is a powerful technology that can reveal more suspicious findings than conventional mammography, such as architectural distortions of breast tissue. But what's the best way to manage these findings?
Researchers led by Dr. Lilian Wang from Northwestern Medicine in Chicago investigated DBT's utility in cases of women who have multiple ipsilateral or contralateral distortions on their scans. While these distortions could be an indication of a high-risk case, they might not necessarily be a sign of malignant disease, they said in a study published July 27 in American Journal of Roentgenology.
"Data from this study demonstrated variation in pathologic outcomes in patients with multiple architectural distortions, leading to complex management decisions," Wang told AuntMinnie.com. "For patients with multiple architectural distortions, biopsy of all areas may be warranted given variation in pathologic diagnoses."
While research has shown that DBT detects more cancers and reduces recall rates compared with conventional mammography, the technology can also reveal subtle findings like architectural distortions that can present interpretation challenges. A 2021 study reported that such distortion on DBT has a pooled positive predictive value (PPV) for malignancy of 34.6%, suggesting that tissue sampling may be needed.
"This becomes problematic in patients with multiple architectural distortions, as it may not be possible or desirable to biopsy all visualized areas," Wang said.
However, managing architectural distortions in patients remains a mystery among radiologists. The researchers noted that there is high interobserver variability in this area and that parenchymal variation may be interpreted as a distortion or as normal parenchyma.
Ultrasound-guided biopsy, MRI, and excisional biopsy with DBT-guided needle localization are a few options that have been suggested. But the researchers found a lack of data addressing histopathologic outcomes in patients with multiple distortions.
Therefore, Wang and colleagues wanted to compare pathologic outcomes between single and multiple architectural distortions identified on DBT.
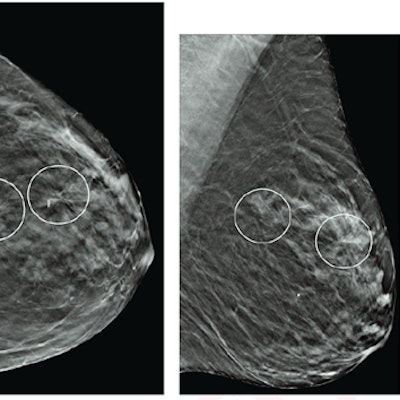
 (A) Craniocaudal and (B) mediolateral oblique DBT images show two areas of architectural distortion in upper outer left breast (circles) that persisted on additional diagnostic tomosynthesis images (not shown). (C) Transverse grayscale ultrasound image of upper outer breast shows irregular hypoechoic mass with associated architectural distortion at 12:30 (arrow), corresponding to posterior architectural distortion. No ultrasound correlate was identified for anterior architectural distortion. Ultrasound-guided biopsy of posterior distortion revealed malignancy (invasive lobular carcinoma). Tomosynthesis-guided biopsy of anterior distortion yielded benign pathology (stromal fibrosis).
(A) Craniocaudal and (B) mediolateral oblique DBT images show two areas of architectural distortion in upper outer left breast (circles) that persisted on additional diagnostic tomosynthesis images (not shown). (C) Transverse grayscale ultrasound image of upper outer breast shows irregular hypoechoic mass with associated architectural distortion at 12:30 (arrow), corresponding to posterior architectural distortion. No ultrasound correlate was identified for anterior architectural distortion. Ultrasound-guided biopsy of posterior distortion revealed malignancy (invasive lobular carcinoma). Tomosynthesis-guided biopsy of anterior distortion yielded benign pathology (stromal fibrosis).The study authors looked at retrospective data for 402 women collected between 2017 and 2019. Out of the total, 372 women had single architectural distortion (145 benign, 121 high risk, 105 malignant, 1 other), and 30 women had multiple visualized distortion. From these two groups, 66 women had biopsied architectural distortion (10 benign, 35 high risk, 21 malignant).
Distortions were characterized as high risk if they had characteristics such as atypical ductal hyperplasia, radial scar, papilloma, flat epithelial atypia, and lobular neoplasia (atypical lobular neoplasia or lobular carcinoma in situ). Malignant distortions were defined as ductal carcinoma in situ (DCIS), invasive ductal carcinoma, and invasive lobular carcinoma (ILC).
| Lesion characterization based on number of architectural distortions on DBT scans | |||
| Single distortion | Multiple distortions | p-value | |
| Benign | 39% | 15.2% | N/A |
| High-risk | 32.5% | 53% | p = 0.002 |
| Malignant | 28.2% | 31.8% | p = 0.56 |
| High-risk + Malignant | 60.7% | 84.8% | p = 0.001 |
Wang et al found that the frequency of malignancy was not different on a statistically significant basis between scans with multiple versus single distortions, on either a per-lesion or per-patient basis. While the frequency of high-risk pathology was significantly higher for multiple than single distortion on a per-lesion basis, it wasn't on a per-patient basis (p = 0.07).
Additionally, the frequency of either high-risk or malignant pathology was significantly higher for multiple than single distortion at both the lesion level (84.8% vs. 60.7%, p < 0.001) and the patient level (93.3% vs. 60.7%, p < 0.001).
The researchers also found that for patient-related characteristics, the presence of single versus multiple distortions was not independently tied to malignancy (p = 0.51). Also, in patients with multiple distortions, the most aggressive pathology across all distortions was not linked to the number of distortions (p = 0.73).
A total of 24 women had two or more ipsilateral biopsied architectural distortions. Out of these, eight saw ipsilateral areas varying in terms of most aggressive pathology. In five out of 10 women with contralateral biopsied distortions, the team found that the contralateral areas varied in most aggressive pathology.
The study authors wrote that these findings may help guide management of architectural distortions visualized by DBT, including multiple distortions. However, Wang told AuntMinnie.com that more data and larger studies are needed to help establish management guidelines in this setting.