In this first installment of a two-part series on implementing postprocessing requirements for radiologists and clinicians in the 3D laboratory, AuntMinnie.com provides 3D technologist Laura Pierce's suggestions on how to address the needs of radiologists.
Radiologists and clinicians often have very different preferences for the postprocessing of 3D images, and a successful 3D laboratory should keep these differences in mind, according to a presentation at the recent International Symposium on Multidetector-Row CT in Washington, DC.
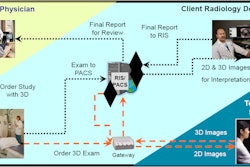
While radiologists need postprocessing for interpretation and need it right away, clinicians are going to view the images for treatment planning and surgical planning, said Laura Pierce, administrative director of the Multidimensional Imaging Processing Laboratory at Duke University.
"They're going to ask you for different views and different product offerings," she said.
The radiologist perspective
If you're creating a new 3D lab or updating an existing lab, it's a good idea to get some verbal input from your radiologists regarding their postprocessing needs, Pierce said. Every section in radiology has different needs.
"You may want to create a 3D steering committee and invite a member from each of your sections to provide you with their input," she said. "You're probably going to get the most input from the cardiovascular section, interventional radiology, and perhaps neuroradiology because they utilize 3D postprocessing the most. But you want to hear from all of the sections in your department."
The next step is to determine your budget, a challenging task because 3D technical reimbursement is now bundled in with CT angiography, MR angiography, and CT charges. A facility's administration will have to calculate the portion of the CT charge to allocate to the 3D postprocessing lab, according to Pierce.
"What you want to do with your usually limited budget is to determine the sweet spot of your highest customer value," she said. "Just provide exactly what your customers need, in this case your radiologists, and that will produce the greatest return for your budget."
A mission and vision for the lab should also be established. This should include the basic tenets of postprocessing: compliance, efficiency, consistency, and quality. Research and teaching could also be added to the list for a teaching institution, Pierce said.
Planners should also determine what imaging modalities the lab would serve. CT will probably be served the most, as CT acquires volumetric datasets. Postprocessing may also be desired for MRI, nuclear medicine, PET/CT, and perhaps volumetric ultrasound datasets.
Lab structure
The structure of the lab is also an important consideration. A centralized 3D lab with trained staff can provide high-quality and efficient images that are very reproducible. It can also provide postprocessing for all satellite sites, Pierce said.
However, postprocessing of some exams -- such as stat studies or anybody going right to the operating room from the scanner -- could be best handled by CT technologists on the scanner console.
"You also may want to provide your 3D service in your reading room," she said. "The 3D can be done by a radiologist in the reading room, or what we have done is site the technologist in the reading room as well. We've found that this improves the communication between the radiologist and the 3D technologist if they're right there."
Pierce noted that 3D enterprise software extends the availability of 3D outside of radiology.
"At our institution, we provide 3D in the operating room, and we're working on providing it on iPads for grand rounds, and also our clinicians are using 3D in their clinics," she said. "They're bringing it up on PACS right now to show their patients the pathology, and it assists them with surgical planning."
Communication is key
This horizontal level of integration requires a tremendous amount of communication, according to Pierce. It's a good idea to staff a 3D lab with an IT service support person, who can make sure all of the equipment is running efficiently across your enterprise and that the same versions of 3D software are being used.
"You also want to make sure that the communications are electronic between all of the sections so that there is no chance of communication errors," she said.
One method of eliciting radiologist feedback is through a survey, although that approach can suffer from low response rates. An online, voluntary survey of radiologists at Pierce's previous institution (Stanford University) elicited 13 responses from eight imaging sections and found a variety of turnaround time expectations. Twenty-three percent expected a postprocessing turnaround time of two to four hours, 31% expected a turnaround time of four to 12 hours, and 31% expected a time of 12 to 24 hours.
Once product offerings for the 3D lab are finalized, it's time to determine staffing needs.
Institutions need to consider exam volume, average exam processing time, and whether to offer radiologists coverage 24/7 or from 8 a.m. to 5 p.m. on Monday through Friday. Acceptable turnaround time should be also defined, so that expectations are very clear and there are no questions on who needs what and when, Pierce said.
3D protocols
The last part of implementing radiologist requests is 3D protocols. There's not a lot of guidance from billing companies about what exactly constitutes a 3D exam, but in 2006 the American Medical Association described complex renderings required for postprocessing: shaded surface rendering, volume rendering, maximum intensity projections, fusion imaging, and quantitative analysis (segmental volumes and surgical planning).
"The one thing missing on that list that's important to radiologists is curved planar reformations," she said.
In summary, all radiologists should be surveyed to get their complete feedback on their postprocessing needs, and a guiding vision and mission should be developed for the 3D lab, Pierce said.
"You want to improve the communication between the 3D lab and your reading rooms," she said. "You want to provide adequate resources to improve turnaround times and you want to develop 3D protocols that will actually add clinical value to the exam for the radiologist."
Part 2 of AuntMinnie.com's coverage of Pierce's talk will highlight the clinicians' perspective on image postprocessing.