NEW YORK CITY - There aren't many hospitals that have 3D imaging services the size of the lab at Massachusetts General Hospital (MGH). Its staff produces advanced visualization images for an average of 2,000 studies each month for its six affiliated hospitals, as well as for external clients of a teleradiology 3D service.
At the New York Medical Imaging Informatics Symposium held September 10, Gordon Harris, PhD, a professor of radiology at Harvard Medical School and the 3D lab's director, described its operation. Advanced visualization has become an integral part of modern radiology and clinical practice, but even with today's technology, producing these images is a specialized discipline.
Massachusetts General Hospital opened its 3D imaging service in February 1999, expanding over the years to offer services to all five Harvard-affiliated hospitals. In 2009, the lab went virtual, offering tele-3D services to hospitals within and outside of the U.S. Additionally, MGH operates the Tumor Imaging Metrics Core (TIMC) of Dana-Farber/Harvard Cancer Center, and maintains the Neurofibromatosis Imaging Analysis Archive. The lab also has a dedicated team of 10 research faculty and fellows who undertake research in 3D imaging.

Click image to enlarge.
Image courtesy of Gordon Harris, PhD.
The lab has three main goals. Its centralized image processing services make rapid-access 3D specialized expertise to any user in the world. It integrates computer-aided detection (CAD) into routine clinical workflow. And it bridges research and clinical advanced imaging applications to migrate new technologies into clinical practice.
The clinical benefits of 3D radiology are undisputed, Harris stated. 3D imaging can reduce the need for exploratory surgery. It can minimize surgical invasiveness and reduce damage to healthy tissues. It can reduce operating room time. A 3D image can provide more comprehensive and realistic views of patients for more intuitive clinical understanding. In some cases, more confident diagnoses and treatment planning decisions can be made.
Secrets of 3D success
The secrets of success behind a 3D lab are training and retaining talented staff, focusing on logistics, aggressively marketing services, and satisfying customers.
For a large lab like that at Mass General, this is a complex task. At least 35 people are full-time employees, and there are additional consultants and collaborators. Fifteen provide clinical 3D imaging and the tele-3D service, including six 3D technologists for CT and MRI, four 3D ultrasound technologists, an image analysis specialist, two administrators, and two technical staff. Ten people support the activities of the Tumor Imaging Metrics Core.
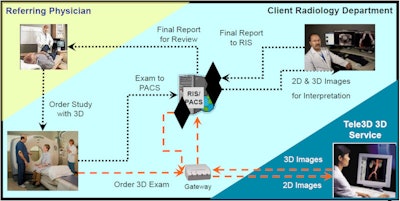
The caveat is that for low-volume 3D labs, it's not cost-effective to maintain the staff, training, and infrastructure required. On average, a case takes an experienced 3D tech between 45 minutes to two hours to process. Rapid turnaround is a necessity. Workflow needs to be tracked, and implementing processes for accurate billing is important. Having full integration with the PACS, information, and billing systems at client hospitals is a key element for success, Harris said.
MGH's 3D image lab internally developed a Web-based radiology order entry system for ordering 3D reconstructions. Exam code identifiers are contained in the RIS to facilitate processing, and there is full DICOM systems integration.
Staffing a lab can also be a challenge. It takes about 12 months to train a 3D technologist, and the dropout rate is about 50%.
|
Advanced visualization techniques
|
"This is a discipline that can be learned, but it's easier to learn and use if a person has an aptitude for the technology," Harris noted. "Not everyone does."
The lab runs 24/7. An extension of the Boston lab is located in Bangalore, India, where a staff of three provide overnight and weekend service. That was established to fill the needs of customers and to eliminate delays in delivering 3D images.
"Running a 3D imaging lab is running a business. It's necessary to develop a business plan, set and achieve financial goals, and do this by making the execution of creating 3D images as efficient as possible," Harris emphasized.
He also noted that the lab needs to work to create an atmosphere in which 3D images are demanded by physicians. Customer satisfaction also is of paramount importance.
Providing clinical trials services
In addition, the lab provides a centralized service to provide standardized tumor measurements for oncology clinical trials. The Tumor Imaging Metrics Core of Dana-Farber/Harvard Cancer Center provides standardized measurements of tumor images acquired by cancer treatment centers participating in clinical trials. This eliminates the problem of inconsistent measurements by different readers, and its centralized image analysis increases reliability.
An online data entry and review system increases efficiency, as does eliminating time-consuming image creation by radiologists at clinical trial sites who are not experienced with 3D image preparation.
TIMC facilitates DICOM transfer from multiple PACS to a secure central database and archive. It can import images acquired from radiology departments that are not active clinical trial participants, either through DICOM CD acquisition or via secure Internet connections. It provides online order entry for authorized users and results that can be viewed by authorized users on a secure website, and its centralized database facilitates internal or external auditing.
After TIMC launched in 2005, it took two years to reach an annual level of 1,000 exams. But between 2007 and 2008, the number of exams processed doubled. The lab now processes nearly 6,000 exams annually. The greatest usage is in phase I clinical trials (14%) and gynecological clinical trials (14%). Breast, gastrointestinal, and sarcoma clinical trials collectively represent another 36%, at 12% each.
TIMC has analyzed more than 30,000 imaging scans and has been used by more than 500 active clinical trials, Harris said. In fact, the budgets of most new clinical trials include funding for TIMC services.
"The growth of our 3D imaging services laboratory has been gratifying. 3D images add a level of visualization that contributes to patient management and complements the grayscale images from which they were created," Harris concluded.