Implementing enterprise-wide 3D capabilities can bring a host of benefits, but the technology requires careful planning to positively affect patient outcomes and financial operations, according to a number of advanced visualization experts.
Within the past few years, software providers have made great strides in upgrading their 3D offerings with technology such as thin-client architecture, allowing clinicians to access and use tools from standard PCs rather than dedicated and expensive workstations.
As part of the justification process for enterprise-wide 3D technology, however, hospital radiology departments and outpatient imaging centers must weigh the long-term value of workflow improvements against the short-term costs of acquisition and clinician behavior modifications, as well as long-term costs of system maintenance, these experts told AuntMinnie.com.
3D's advantages
The primary advantage of enterprise-wide 3D is the ability to view and interact with 3D images from anywhere within an institution or even outside its walls, providing improved service to referring physicians, better communication with patients, and enhanced collaboration capabilities, said Gordon Harris, Ph.D., director of 3D imaging service at Massachusetts General Hospital (MGH) in Boston
Typical enterprise-wide 3D, which Zaffar Hayat, president of Viatronix in Stonybrook, NY, labels "general-purpose 3D," offers the reading radiologist or physician "great flexibility." Furthermore, he added, PACS companies have made a majority of daily exams accessible and available on an enterprise basis.
Such a "virtualized workflow" that routes imaging studies to clinicians at any location "can significantly shorten turnaround time and speed the delivery of reports since any available radiologist can read the exam, even if they are offsite," according to Eddie Moore, a digital solutions architect at Carestream Health in Rochester, NY.
Images in 3D form have become essential as a clinical diagnosis and interventional planning tool, said Ray Ghanbari, Ph.D., executive vice president of strategy and products at Vital Images in Minnetonka, MN.
"Providing these tools across the enterprise gets these images right to the point of care, right to the point in time that critical decisions are being made," Ghanbari said. "Using the Web-client technology means that all the clinical tools can be available everywhere and that desktop hardware and workstation licensing is not an obstacle to hospital planners."
But those interested in enterprise-wide 3D may face high costs and technical limitations, Harris said.
"Some systems have requirements for high-resolution monitors, which may not be available at all office or offsite locations," he noted. "Also, there may be lag time in responsiveness if the client and server are widely separated, or if the connection is low bandwidth."
Adding more workstations only multiplies the cost of maintenance for software, hardware, and IT infrastructure, as well as "the hassle of having to deal with network issues related to data/image transfer," Harris continued.
Instead, Viatronix's Hayat encouraged those interested in enterprise-wide 3D to apply the technology to a selection of clinical specialties, such as cardiac CT angiography (CTA), CT colonography, and vascular analysis, that do not necessarily require a thin-client-type interface or a read-from-anywhere scenario.
 |
| Some specialized clinical applications such as CT cardiac analysis can be made available on a limited number of workstations, making 3D more economical across the healthcare enterprise. Image courtesy of Viatronix. |
Before acquiring enterprise-wide 3D capabilities, clinicians should ask this fundamental question: "Is it necessary to purchase and maintain a clinical application across a wide-area network when it is only used by a few highly specialized physicians within the group?" Hayat said.
Vital Images' Ghanbari said that the "truly disruptive" nature of the technology itself may cause some to be cautious about adoption and implementation.
"There is a tremendous opportunity to recast the whole workflow, optimized around the clinical questions," he said. "But this requires retooling physician expectations that have been built around a workstation, and retooling the infrastructure required to provide universal enterprise access to these capabilities."
Generating value
Greater workflow flexibility and enhanced productivity for radiologists and referring physicians who can view 3D images remotely yield a competitive advantage for organizations, according to Carestream's Moore. Such benefits include radiology reports that contain links to key 3D images or to the entire exam, enterprise user licensing versus purchasing a separate license for each 3D user, and no need for expensive, dedicated 3D workstations.
 |
| Enterprise-wide 3D can deliver value in a wide variety of clinical situations. Image courtesy of Carestream Health. |
Harris targeted three areas where enterprise-wide 3D generates value. The first involves a setting where multiple groups must collaborate, such as in cardiac CTA, where the 3D lab will preprocess an exam that the cardiovascular radiologists and cardiologists will read interactively and work together to assess.
The second involves remote operations and review. These include on-call, offsite decision-making and where multiple institutions work together on a single patient.
"A patient at one site may need to be transported to another site for trauma care, and a review at the remote site is needed to decide whether to move the patient," he noted.
The third involves remote interactive 3D capability, such as that used by MGH's Tele3D Advantage 3D imaging service for other hospitals and imaging centers, Harris said.
CT angiography makes 3D visualization and related tools an "absolute necessity," said Ghanbari, who also sees 3D visualization gaining in popularity among other high-end workflows ranging from lung nodule examination to evaluation of ischemic stroke.
|
Enterprise-wide 3D aids in decisive surgical calls More radiologists and referring physicians may be pursuing enterprise-wide 3D visualization capabilities, but their preference for such advanced technology isn't just about having the coolest tools in their clinical arsenal. It's about surgical outcomes with the patient as top priority. For example, a surgeon at Illinois Masonic Medical Center in Chicago used 3D tools from Vital Images to visualize a large sarcoma on a patient's hip, recalled Ghanbari. As a result, the surgeon was able to visualize the internal iliac artery in relation to the tumor, which provided him with the confidence to proceed with the surgery, and the 3D views of the muscles and tumor margins determined the strategy for the resection, Ghanbari said. In another case, 3D may have saved a patient's life, according to Moore. A patient who had six toes on one foot was having surgery to remove the extra toe, he said. "Normally the outside toe would be removed. As the patient entered the surgical suite, the surgeon looked at the imaging study in vessel-tracking mode," Moore said. "He could see that a large artery was wrapped around the outside toe. That artery posed a major surgical risk, so an inner toe was removed instead." |
"A small covey of specialized workstations from various vendors, spread across a few of the reading rooms or hidden in a 3D lab, are no longer sufficient," he said. "The workload has flushed these out into the open, and, as such, they need to be integrated as core tools so that every diagnostic user can access them in a common and consistent way."
Referring physicians are also increasingly taking an active role with 3D, according to Ghanbari.
"The referring community is no longer satisfied with a static image in a PACS and a disconnected reference in the report," he said. "They know these tools exist and are demanding real-time access to interactive 3D and decision support. Referring physicians have an expectation that they can step directly into the 3D content along with the radiologist."
Referring physicians increasingly are demanding 3D and 4D or functional imaging, which not only opens up a new range of applications but also creates new demands and complexity for visualization products and infrastructure, he added.
PACS appeal
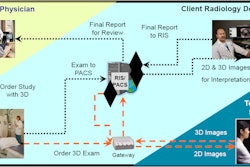
One of the primary workflow issues with enterprise-wide 3D visualization revolves around its interaction with PACS, whether via an interface or full integration.
In one case, clinicians launch the 3D server application directly from the PACS worklist. Clinicians may also launch the application from the radiology worklist or independently by logging directly into the 3D system, according to Harris.
"One of the workflow issues is that images that might need 3D review must be pushed to the 3D server as well as to PACS, which increases network traffic and requires rules determining which images should go to the 3D server," Harris said.
Typically, the PACS serves as the data source for 3D imaging datasets, said Henri "Rik" Primo, national director of marketing and strategic relationships for Siemens Healthcare's Image and Knowledge Management unit in Malvern, PA. The CT or MR modality sends images to PACS, and a 3D viewer is launched on the images residing in the PACS.
"Some institutions prefer to perform the 3D reconstructions by the radiologists or clinicians at a PACS workstation; others rely on a 3D lab where well-trained [radiologic technologists (RTs)] are performing the 3D reconstruction," Primo said. "After processing, the RT is then forwarding the 3D images to the patient folder in the PACS."
"Separate workstations for PACS and 3D can complicate the workflow," Primo said, distracting the clinician because he or she has to walk from one workstation to another, select the patient and exam again, perform 3D, and then return to the PACS workstation. As a result, equipping a single workstation with both 3D and PACS has its advantages, he added.
In a centralized model, the thin-slice data only have to be sent to one location and do not have to flood the PACS archive, according to Chris Petillo, senior director of ancillary systems, information technologies, at New York University Langone Medical Center in New York City.
"Once the data are manipulated, the output, which is a much smaller dataset, can then be sent to the PACS and clinical distribution system for access from the radiologist or referring clinician," he said.
Ghanbari emphasized that advanced clinical workflows "dovetail" with the PACS.
"In an ideal implementation, the user can seamlessly move from a traditional PACS interaction to the 3D," he said. "Sharing patient context with the PACS worklist and ensuring that intermediate results and key images are automatically stored in the archive is ideal. It is important to think of these results as more than simple images, but more importantly as living interactive evidence that is created, edited, and reviewed as it flows back and forth between technologist, radiologist, and referring physician over the course of a patient's ongoing medical treatment."
But the system also must be easy to use, with a scalable, enterprise-ready infrastructure so that it supports the analytic complexity and data volumes associated with large 3D datasets, he stressed.
Changing roles
Enterprise-wide 3D not only alters the workflow of radiologists and referring physicians, but also the roles of both in terms of their ongoing interaction, experts indicated.
"Radiologists gain tremendous productivity because they no longer need to go to a dedicated workstation to read 3D exams," Moore noted. "They can also spend more time reading and less time performing image set-up and other administrative tasks. They can bring up a 3D view with just a couple of clicks, read the exam, identify and attach key images, and dictate the report."
In addition, media-rich reports can be delivered quickly to referring physicians and can contain key images that make it fast and easy for the referring clinician to view the anatomy and any measurements or annotations, he said. Such tools to use during patient consultations can boost referral loyalty, he added.
Certainly, enterprise-wide 3D usage improves communication and collaboration between the two roles, according to Ghanbari.
 |
| Many enterprise-wide 3D proponents believe the technology can facilitate collaboration between radiologists and referring physicians. Image courtesy of Vital Images. |
"Enterprise-wide 3D postprocessing using thin-client technology allows for a much better relationship between radiology and the referring physicians," Petillo said.
"Data are available to the clinicians faster, and real-time consultation can be done while all parties are reviewing the images -- from anywhere in or even out of the facility," he said.
Enterprise-wide 3D capabilities may eliminate telephone conferences, particularly between physicians and radiologists in complicated ER or ICU cases, according to Primo. "With a Web-based 3D viewer, all involved physicians can look at the 3D images simultaneously and consult, whether they are located in the radiology department, ICU, OR, emergency department, or at home," he noted. "It's a real-time experience between the radiologists and the referring clinicians. This facilitates accurate and quick care."
Furthermore, there are relationships among anatomical structures that can't be seen very well with standard axial imaging, Primo continued, but thin-client 3D brings this capability to clinicians like neurosurgeons, oncologists, and orthopedic surgeons.
Enterprise-wide 3D can have both positive and negative impacts on the roles of the radiologist and referring physician, Harris said.
"If the site has a 3D lab to preprocess the images, the radiologist can then interact with the images created by the lab, or for urgent review, can do a quick interactive review for an initial impression and then refer to the fully processed views from the 3D lab for a final report," Harris said.
"Without a 3D lab," he continued, "having access to interactive 3D can improve a radiologist's diagnostic confidence and allow some quick overview, but doing all the 3D processing may require more time than the radiologist wants to spend per case, and, thus, 3D access in the absence of dedicated 3D technologists can enhance as well as hinder productivity, depending on the proficiency of the particular radiologist in using the 3D software."
Any decision to implement enterprise-wide 3D carries tremendous ramifications, Ghanbari said.
"Implemented well, enterprise solutions enable the hospital to rethink the workflow from a clinical perspective, rather than being caught in a medical assembly line paradigm from order to report," he said. "Integration with the archive and information systems lets users design the appropriate clinical flow for all the scenarios from supervised radiology residents to time critical stroke intervention cases. Implemented poorly with technologies not built for the enterprise, the complexity of managing large 3D datasets can bring workflows, systems, and networks to the breaking point."
By Rick Dana Barlow
AuntMinnie.com contributing writer
June 2, 2009
Related Reading
Turning your 3D lab into a profit center, May 21, 2009
3D technologists: You've trained them -- now retain them, August 15, 2007
Navigating the economics and billing of advanced visualization, May 17, 2007
Radiologists may be better off taking hands-on approach to 3D workflow, April 30, 2007
How to find and train a 3D technologist, June 17, 2005
Copyright © 2009 AuntMinnie.com