Researchers from South Korea have developed a technique to enhance the safety of robotic thyroidectomy by overlaying augmented reality (AR) models, based on CT scans, directly onto patients during surgery, according to a study published in the December issue of Annals of Surgical Treatment and Research.
Robotic surgery is often the technique of choice for thyroidectomy due to its high efficiency and minimally invasive nature, compared with conventional open surgery, noted co-first authors Dongheon Lee from Seoul National University and Dr. Hyoun-Joong Kong from Chungnam National University Hospital. However, the advanced surgical method is challenging because it provides a limited operative view of neighboring structures that are covered by tissue and have no means of palpation, which increases the potential for complications such as tracheal perforation.
To overcome these obstacles, Lee, Kong, and colleagues applied augmented reality to robotic surgery, particularly hoping to enhance the visualization of otherwise hidden structures during thyroid resection (Ann Surg Treat Res, December 2018, Vol. 95:6, pp. 297-302).
"Incorporation of AR in laparoscopic or robotic surgery aids the surgeon to more easily perceive anatomical structures intuitively which helps to identify structures covered or hidden by surrounding tissue," they wrote.
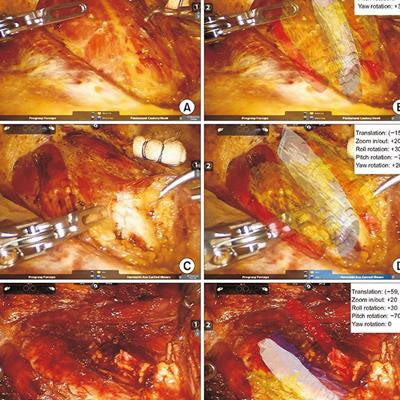
 Clinicians can overlay 3D virtual models onto patient anatomy during thyroid surgery with augmented reality technology. Image courtesy of Lee et al. CC BY-NC 4.0.
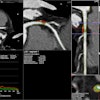
Clinicians can overlay 3D virtual models onto patient anatomy during thyroid surgery with augmented reality technology. Image courtesy of Lee et al. CC BY-NC 4.0.The researchers acquired a CT scan of the thyroid gland, carotid arteries, trachea, and esophagus of a 45-year-old patient with papillary thyroid cancer. Using open-source computer software, they segmented and processed the imaging data to generate 3D virtual models compatible with AR software. They also used the same imaging data to create a multicolored 3D-printed model.
Before applying the AR model to surgery, the group superimposed it onto the patient-specific 3D-printed model using proprietary image registration software to determine the accuracy of the AR model. Image registration between the organs and vessels of the AR model and those of the 3D-printed model was highly accurate, with an average Dice similarity coefficient of 0.987 when viewed from five different angles.
Following this validation protocol, Lee, Kong, and colleagues used their augmented reality technique in conjunction with a robotic surgical machine (da Vinci surgical system, Intuitive) for actual left thyroid lobectomy.
They first overlaid the AR model onto the patient's neck muscles to display the approximate location of the thyroid and nearby underlying organs. After moving the muscles aside, the clinicians directly aligned the AR model with its corresponding structures, enabling the operating surgeon to see, in real-time, virtual models of surrounding organs and vessels that were hidden behind tissue.
The surgeon successfully completed the procedure while periodically referencing the AR model on a separate monitor. Though the AR technique allowed for the safe execution of thyroidectomy, it also increased surgical time because of the need to reset image registration whenever the surgeon changed operative angles.
"Organs that should be protected during robotic thyroidectomy were clearly visualized using AR based on preoperative CT images," the authors wrote. "Although current AR in robotic thyroidectomy has limited clinical applicability due to technical and commercial limitations, AR in robotic surgery has several advantages that may enhance surgical safety."