While the implementation of PACS in radiology brought a host of clinical benefits, it came with a downside: less interaction between radiologists and clinicians. An iPad application developed by a Johns Hopkins team offers the promise of recapturing the clinical and educational value of frequent face-to-face consultations.
Called Radiologists Engaging and Collaborating in Healthcare, or REACH, the application's user interface combines a Web-based PACS viewer, access to radiology reports, and videoconferencing. It allows radiologists and clinicians to consult and collaborate in real-time using their iPads, breaking down current barriers to consultations, according to Dr. Paras Khandheria of Johns Hopkins Hospital.
He presented the project during a scientific session at the recent Society for Imaging Informatics in Medicine (SIIM) meeting in Long Beach, CA. The study won the Roger A. Bauman, MD Award for best student paper at the conference.
The old days
In a traditional specialist consultation model, a patient is referred to a specialist. After the specialist assesses the patient, any additional testing and workup is performed, Khandheria said. The specialist then renders an assessment and plan in conjunction with the patient's primary physician.
In the old days, clinicians -- who didn't have access to imaging studies -- had to come down to the radiology department to formulate a plan in conjunction with the radiologist. That's changed, obviously, with PACS; clinicians can now view images remotely and correlate with the written report as needed.
"Radiology has become a little bit of a black box, in which [clinicians] just get an output and go based on that," he said.
Multiple studies haves shown significant decreases in personal consultations between clinicians and radiologists after adoption of enterprise-wide PACS. Because clinicians now have remote access to images, they no longer have to speak to the radiologist.
"No one would argue that PACS on balance has been a great thing for the field of radiology; it's dramatically increased efficiency and ease of delivery. But have we lost something?" he asked. "Is there a deficiency now with the current way we provide radiology services? And the million-dollar question is: Has it affected patient care?"
Radiologists can significantly improve the clarity of their findings if they can point out and explain their findings to clinicians, Khandheria said.
Preventing communication breakdown
The importance of consultations can't be understated; communication breakdown is a major causative factor in radiology malpractice litigation. These consultations also benefit both radiologists and clinicians, he said.
"The radiologist [gains] a better ability to apply clinical findings to the study, and the clinician [can grasp] the imaging abnormalities with a deeper understanding, and can understand the implications for patient management and [determine] if other workup is indicated," Khandheria said.
While clinicians can reach radiologists via pager and phone if they have questions, the phone doesn't allow a visual review of findings. Email lacks immediacy and also doesn't facilitate visual correlation during consultation, he noted.
The best form of consultation is face to face, but it's not always easy to arrange that in practice.
"It takes time on the part of the clinician and the radiologist; you have to coordinate the availability of both parties," he said. "The radiology department may be way down in the basement, and the clinician may be on a different part of campus. Sometimes that contributes to a lack of personal relationships; the clinician has no idea who you are, even though you've read [studies] on their patients for months now."
New consultation model
The Johns Hopkins team developed REACH in an attempt to improve this situation. The iPad application's interface combines an enterprise-grade Web-based PACS viewer, radiology report text fetched from the RIS, and real-time audio/video teleconferencing.
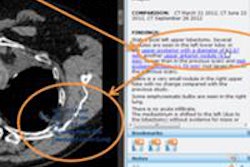
 Screenshot of REACH. The top left-hand corner demonstrates the active videoconferencing session, while the bottom left of the screen shows the radiologist report associated with the study. The right side of the screen contains the study itself, loaded into an HTML5 lightweight PACS viewer. Image courtesy of Dr. Paras Khandheria.
Screenshot of REACH. The top left-hand corner demonstrates the active videoconferencing session, while the bottom left of the screen shows the radiologist report associated with the study. The right side of the screen contains the study itself, loaded into an HTML5 lightweight PACS viewer. Image courtesy of Dr. Paras Khandheria.REACH supports shared PACS session management, which allows any changes made to one viewer -- such as selection of series/slices, window settings, zoom, measurements, or annotations -- to be instantly propagated to the other viewer, Khandheria said.
"If the clinician scrolls to a different part, points to something, and says, 'What is this?' the radiologist knows unambiguously what they're pointing to and can do the same thing for the clinician," he said. "Both parties are seeing exactly the same thing."
The hypothesis behind REACH is that a visual-rich conversation via a teleconsultation system is superior to an audio-only discussion in terms of clinical care and education, Khandheria said. Also, a video conversation builds rapport between the radiologist and clinician, improving the chances for collaboration in the future, he said.
Workflow
If a radiologist is available for consultation, he or she activates REACH on an iPad and then resumes daily work. Clinicians who have a question regarding a radiology study during their review of clinical data can then activate REACH on their iPad. They load the study in question, identify an available radiologist, and request a consult via REACH, Khandheria said. The radiologist receives the request and can accept the consult or decline it, with the option of a sending a message back to the clinician.
The goal of REACH is to lower the barrier to consultations between radiologists and clinicians, he said. Khandheria is currently the only radiologist using REACH clinically, but the institution is planning a wider deployment of the system, with radiology residents serving as a "call pool" for consultation on studies.
"Hopefully we'll have benefits to both the radiologist and clinician and drive improvements in patient care," he said.