Adrenergic Nervous System of the Heart
Physiology & Pharmacology
The sympathetic and parasympathetic innervation of the heart plays a major role in the regulation of cardiac function [14]. Adrenergic fibers that innervate the heart originate in the left and right stellate ganglia [9]. The left stellate innervates the right ventricle, whereas the right stellate innervates the anterior and lateral portions of the heart. The adrenergic fibers travel in the subendocardium following the coronary vessels [9]. At a cardiac level, sympathetic activation results in an increased heart rate (chronotropic effect), augmented contractility (inotropic effect), and enhanced atrioventricular conduction [9].
Sympathetic nervous system dysfunction plays a role in heart failure [18]. Both increased neuronal release of norepinephrine and decreased efficiency of NE uptake contribute to increased cardiac adrenergic drive [18]. Significant reduction in mortality in heart failure patients can be achieved with the use of beta- and alpha-adrenoreceptor blocking drugs [18].
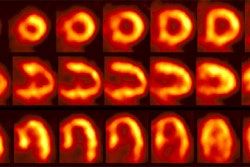
I-123 MIBG has been used to study the cardiac sympathetic nervous system because of its high cardiac uptake. Non-neuronal activity clears rapidly from the heart between 15 and 60 minutes. In the heart, MIBG is taken up by the postganglionic, presynaptic nerve endings [21]. As for norepinephrine, I-123 MIBG uptake is predominantly mediated (70%) via an energy dependent, type I uptake mechanism [9]. After depolarization MIBG is released into the synaptic cleft, like norepinephrine, but it is not further metabolized [21]. MIBG stored within the neuron is also not further metabolized (it is not a substrate for monoamine oxidase) and only about 10% of the dose is altered after several days, primarily by deiodination. The agent produces no measurable pharmacologic effects. Uptake of I-123 is usually homogeneous within the myocardium, although uptake may become more heterogeneous or decrease within the inferior (men) or lateral (woman) wall as the patient ages [1,2]. Tracer washout also increases with increasing age [2].
Technique:
The dose used for the exam is 3 to 10 mCi of I-123 MIBG [8,9,13]. Patients should fast for 6 hours prior to the exam [13]. Thyroid uptake is blocked by the oral administration of 500 mg potassium perchlorate (Lugols solution) or a saturated solution of potassium iodide given 30 minutes before injection of the radiotracer [20]. Early (10-20 minute post injection) and delayed (4 hour) planar and SPECT imaging is performed. A low-energy parallel hole collimator is used for imaging [20]. A 20% window is used and centered over the 159 keV I-123 photon peak [9,20]. An anterior planar image of the chest is acquired for 5 minutes prior to initiation of SPECT imaging using a 128x128 matrix (some centers also acquire a planar LAO image [9]). SPECT images are obtained every 6 degrees for 30-40 seconds in a 64x64 matrix for a 180 degree rotation (RAO to LPO).
Findings:
In healthy subjects, MIBG uptake is slightly lower in the inferior wall (likely due to attenuation) and apex [14]. MIBG uptake is semiquantified by calculating a heart-to-mediastinum ratio on the planar images [15]. The anterior projection seems to be the preferred projection for quantification as it provides the lowest variation and highest resolution [19]. Various methods have been described. In one method a 7 x 7 pixel ROI is placed over the cardiac region and another 7 x 7 pixel ROI over the upper mediastinal area [13]. In another method, left ventricular activity is measured by manual drawn regions of interest surrounding the entire myocardium (excluding ventricular blood pool) [15]. A separate 20 x 20 pixel region of interest is placed over the upper mediastinum. The heart-mediastinum ratio is calculated without background subtraction as mean (or average) counts per pixel over the left ventricle divided by mean (or average) counts per pixel in the upper mediastinum [9,15].
A heart-to-mediastinum ratio of greater than 1.8 is considered normal [9]. The clearance rate from the myocardium (washout rate) is calculated by: (Initial myocardial MIBG uptake - Delayed myocardial MIBG uptake/ Initial MIBG uptake) x 100 [13]. The washout rate between early and delayed images should be less than 10% [9]. Non-uniform soft tissue attenuation over the chest can cause variations in the measurements obtained [9].
In healthy subjects, there is low within subject variability in I-123 MIBG uptake on both planar (about 5%) and SPECT (about 5%) imaging [19]. Assuming this is also true for patients with cardiac disease, the effects of therapeutic interventions can be monitored using I-123 MIBG imaging [19].
In cardiomyopathies/heart failure:
In patients with heart failure the assessment of sympathetic activity has important prognostic implications and will result in better therapy and outcome [10]. Alterations in the cardiac sympathetic nervous system clearly play a role in the development and progression of congestive heart failure (CHF) [13,15]. Decreased cardiac output related to left ventricular dysfunction results in a baro-receptor mediated increased in sympathetic tone and circulating norepinephrine levels [15]. The consequences of chronically increased sympathetic tone include increased left ventricular afterload, worsening LV function, and progressive CHF [15]. Additionally, in CHF patients the postsynaptic beta1-adrenoreceptor density is reduced and the concentration of inhibiting Gi-alpha proteins is elevated [13]. Cardiac noradrenaline turnover is also increased [13]. Beta-adrenergic blocking agents can aid in blocking sympathetic overstimulation associated with CHF [15].
Cardiac MIBG uptake is generally diffusely decreased in patients with dilated cardiomyopathies (defects in patients with ischemic cardiomyopathies tend to be more severe in necrotic segments) [11,14]. In these patients, low MIBG uptake is associated with an increased risk for cardiac death [9,11,14,15]. Decreased MIBG uptake on delayed images is closely related to the degree of LV dysfunction in patients with heart failure and also correlates with the level of decreased exercise capacity [8,16]. The poor tracer uptake is likely reflective of underlying cardiac autonomic dysfunction which may place patients at higher risk for arrhythmogenesis [11]. Improvement in MIBG uptake following initiation of beta-blocker therapy may predict which patients are more likely to respond to this form of therapy- even prior to documented LV function improvement [14].
Tracer washout rates have also been studied. Patients with dilated cardiomyopathies typically have accelerated washout rates of MIBG of greater than 25% between early and delayed images (normal less than 10%) [9]. A washout rate of greater than 50% is also associated with an increased risk for cardiac death [9,11]. Increased washout can also be seen in other conditions including myocardial hypertrophy and diabetic hearts [11]. MIBG uptake ratios may also help to predict a good response to alpha-blocker therapy in patients with dilated cardiomyopathies [9].
Cardiac resynchronization therapy (CRT) has been shown to be beneficial in patients with advanced chronic heart failure and a QRS duration greater than 120 milliseconds [22]. CRT can improve clinical manifestations and quality of life and reduce complications and risk of death [22]. Lower MIBG uptake (H/M ratio below 1.36) is associated with a higher likelihood for lack of response to CRT [22]. The lower MIBG uptake may reflect hearts with more severe myocardial damage that are less likely to respond to CRT [22]. Following successful CRT intervention, there is improved cardiac uptake of MIBG [22].
Patients with hypertrophic cardiomyopathies also demonstrate derangements in sympathetic activity [12]. HCM is an inherited cardiac muscle disease that is related to a mutation in the genes that encode proteins in the sarcomere [12]. Charateristics of the disorder include disproportionate left ventricular hypertrophy and diastolic dysfunction [12]. Delayed MIBG images demonstrate poor, heterogeneous cardiac tracer retention and increased washout rates [12].
In heart transplantation:
The surgical procedure of heart transplantation causes autonomic denervation of the donor (allograft) heart [7]. Immediately after heart transplantation no activity is detected in the myocardium [14]. Total denervation persists for at least 12 months after transplantation [14]. Regional reappearance of sympathetic nerve fibers occurs in the transplanted heart over time [7]. MIBG uptake indicating partial sympathetic reinnervation can be shown in 40% of patients 3 to 5 years after transplantation [7]. Serial MIBG studies show that reinnervation begins from the anterolateral base of the heart and spreads towards the apex [9,14]. With reinnervation, patchy MIBG uptake is seen primarily in the anterior, anterolateral, and septal regions. MIBG uptake is usually not apparent in the posterior or inferior myocardial regions, except for basal posterior localization [9]. Complete reinnnervation of the heart is not seen- even up to 12 years after transplantation [9].
In myocardial infarction/ischemia:
Uptake of I-123 MIBG is decreased in areas of acute and chronic ischemia [9].
Myocardial infarction destroys the myocardium and the nervous tissue in the myocardium. However, in the early post-infarction period, the MIBG defect is typically larger than the area of infarcted myocardium (a perfusion-innervation mismatch) [9,14]. This is because infarction can result in destruction of proximal neurons which supplied innervation to distal areas in which myocardial tissue is still viable [14]. As a result of this, a defect identified on MIBG scintigraphy following infarction, may be more extensive than the actual area of infarction as demonstrated by thallium. Denervated, but viable myocardium has been shown to be supersensitive to catecholamines and this may explain an increased risk for arrhythmogenicity in certain patients following MI [14]. Reinnnervation to these peri-infarct regions can be demonstrated by reappearance of MIBG uptake usually within 14 weeks following the cardiac event [9]. Unfortunately, reinnervation may be incomplete [9].
Conditions which decrease cardiac MIBG uptake
- Pheochromocytomas/Elevated circulating levels of MIBG (due to excess circulating norepinephrine which competes with MIBG for the type I uptake system)
- After eating
- Administration of yohimbine (due to increased adrenergic activity)
- Administration of tricyclic antidepressants (imipramine, desipramine)
- Administration of sympathomimetics (pseudoephedrine or phenylpropanoloamine)
- Cardiovascular autonomic neuropathy of diabetes mellitus: Cardiovascular autonomic neuropathy is a serious complication of diabetes and the prevalence can be as high as 20-30% of patients with non-insulin dependent diabetes (NIDDM) [21]. Decreased cardiac MIBG uptake in diabetic patients is associated with an increased mortality [9,21]. Improvement in glycemic control has been shown to result in partial restoration of sympathetic innervation [14].
- Following cardiac transplantation (within 1 year, beyond this time about 50% of patients may demonstrate uptake indicative of re-innervation)
- Following ascending aortic aneurysm surgical repair- most likely the result of mechanical damage to the cardiopulmonary nerves surrounding the aorta [10].
- Following chemotherapy with doxorubicin: Decreased myocardial MIBG uptake can be seen following doxorubicin therapy, with limited morphologic damage [9]. Decreased MIBG uptake follows a dose dependent decline with about 25% of patients demonstrating some decrease in MIBG uptake at cumulative doses of 240-300 mg/m2 [9]. Decreased MIBG uptake precedes deterioration of ejection fraction [9,14]. Evidence of sympathetic damage can be used to select patients at risk of severe functional impairment and who may benefit from cardioprotective agents or changes in the schedule of antineoplastic drugs [9].
- Congestive heart failure secondary to pressure or volume overload
- Dilated cardiomyopathy- washout is also increased in these patients [6]
- Acute Myocarditis [6]
- Myocardial infarction [6]
- Sympathetic nerve destruction by stellate ganglionectomy
- Epicardial phenol application, and Shy-Drager syndrome.
- Parkinson's disease [10,14]. MIBG abnormalities observed in Parkinson's patients may be due to postgangliotic sympathetic dysfunction and has been correlated with severity and length of disease [14].
- LV hypertrophy due to essential hypertension [14]. MIBG abnormality is mainly observed in the inferior and lateral walls and the degree of abnormality correlates with the severity of hypertrophy [14].
Conditions which increase cardiac MIBG uptake
- Administration of clonidine (an alpha-2 antagonist which slows nerve traffic)
- Heart failure secondary to coronary artery disease
REFERENCES:
(1) J Nucl Med 1995; Tsuchimochi S, et al. Age and gender differences in normal myocardial adrenergic neuronal function evaluated by iodine-123-MIBG imaging. 36: 969-974
(2) J Nucl Med 1998; Sakata K, et al. Physiologic fluctuation of the human left ventricle sympathetic nervous system assessed by Iodine-123-MIBG. 39: 1667-1671
(3) Nucl Med Annual 1993; Sisson JC. The adrenergic nervous system of the heart and nuclear medicine. Ed. Freeman LM. Raven Press, NY.: 233-249 (No abstract available)
(4) J Nucl Med 1995; Mantysaari M, et al. Myocardial sympathetic nervous dysfunction detected with iodine-123-MIBG is associated with low heart rate variability after myocardial infarction. 36: 956-61
(5) J Nucl Med 1995; Glowniack JV. Cardiac studies with metaiodobenzylguanidine: a critique of methods and interpretation of results. 36: 2133-37 (No abstract available)
(6) J Nucl Med 1998; Agostini D, et al. Impariment of cardiac neuronal function in acute myocarditis: Iodine-123-MIBG scontography study. 39: 1841-1844
(7) J Nucl Med 2001; Odaka K, et al. Reappearance of cardiac presynaptic nerve terminal s in the transplanted heart: Correlation between PET using 11C-hydroxyephedrine and invasively measured norepineephrine release. 42: 1011-1016
(8) J Nucl Med 2001; Zhao C, et al. Comparison of cardiac sympathetic nervous function with left ventricular function and perfusion in cardiomopathies by 123I-MIBG SPECT and 99mTc-Tetrofosmin electrocardiographically gated SPECT. 42: 1017-1024
(9) J Nucl Med 2001; Carrio I. Cardiac neurotransmission imaging. 42: 1062-1076
(10) J Nucl Med 2001; Momose M, et al. Total and partial cardiac sympathetic denervation after surgical repair of ascending aortic aneurysm. 42: 1346-1350
(11) J Nucl Med 2001; Wakabayashi T, et al. Assessment of underlying etiology and cardiac sympathetic innervation to identify patients at high risk of cardiac death. 42: 1757-1767
(12) J Nucl Med 2002; Shimizu M, et al. Heterogeneity of cardiac sympathetic nerve activity and systolic dysfunction in patients with hypertrophic cardiomyopathy. 43: 15-20
(13) J Nucl Cardiol 2002; Parthenakis FI, et al. Segmental pattern of myocardial sympathetic innervation in idiopathic dilated cardiomyopathy: relationship to regional wall motion and myocardial perfusion abnormalities. 9: 15-22
(14) J Nucl Cardiol 2002; Patel AD, Iskandrian AE. MIBG imaging. 9: 75-94 (No abstract available)
(15) J Nucl Cardiol 2002; Gerson MC, et al. Carvedilol improves left ventricular function in heart failure patients with idiopathic dilated cardiomyopathy and a wide range of sympathetic nervous system function as measured by iodine 123 metaiodobenzylguanidine. 9: 608-615
(16) J Nucl Med 2003; Sato M, et al. Correlation between cardiac norepinephrine overflow during exercise and cardiac 123I-MIBG uptake in patients with chronic heart failure. 44: 1618-1624
(17) J Nucl Med 2003; Inoue Y, et al. Effect of collimator choice on quantitative assessment of cardiac iodine 123 MIBG uptake. 10: 623-32
(18) J Nucl Cardiol 2003; Narula J, Sarkar K. A conceptual paradox of MIBG uptake in heart failure: retention with incontinence. 10: 700-704
(19) J Nucl Cardiol 2004; Somsen GA, et al. Normal values and within-subject variability of cardiac I-123 MIBG scintigraphy in heathy individuals: implications for clinical studies. 11: 126-133
(20) J Nucl Cardiol 2004; Flotats A, Carrio I. Cardiac neurotransmission SPECT imaging. 11: 587-602
(21) J Nucl Cardiol 2006; Mushtaq N, et al. I-123 metaiodobenzylguanidine imaging in non-insulin-dependent diabetic patients with normal myocardial perfusion scans: new insights into their increased cardiac morbidity and mortality rates. 13: 8-10
(22) J Nucl Cardiol 2007; D'Orio Nishioka SA, et al. Cardiac sympathetic activity pre and post resynchronization therapy evaluated by 123I-MIBG myocardial scinitgraphy. 14: 852-859