Bone Imaging in the
Post-operative Patient:
Post-operative
Evaluation of Spinal Fusion:
Spinal fusion is performed in patients with back pain due to segmental instability. Persistent back pain in the first few years after the procedure is often related to failure to achieve structural integrity of the fusion (pseudoarthrosis). The incidence of pseudoarthrosis following spinal fusion varies from 10 to 30%, however, not all patients with pseudoarthrosis suffer from back pain. Early failed fusion is usually treated with repeat surgery. Bone scanning can be used to detect the presence of a pseudoarthrosis in patients with continued pain following spinal fusion. On SPECT images successful fusions demonstrate diffuse, but not increased, uptake which can be inhomogeneous, and no evidence of focal abnormalities within the fusion mass. This uptake is probably due to widespread new bone formation. Uptake within the vertebral bodies or apophyseal joints at the fusion levels may be seen and are more common with posterior fusions. These findings may be due to motion within the fusion, despite the absence of pseudoarthrosis. Due to the alterations in impact loading following fusion, focal uptake in the vertebral bodies and apophyseal joints in the free motion segments adjacent to the fusion are commonly seen: 45% of patients following lateral fusion and 87% of patients following posterior fusion (posterior fusion has been shown to produce greater stress in the free segments adjacent to the fusion). A pronounced focal increase in uptake within the fusion mass more than 1 year post-op is highly suspicious for pseudoarthrosis. Generally, significant healing of the fusion is complete by 6 months, but as at other sites of surgery, scintigraphy may remain positive for up to 2 years. As a general rule if healing is taking place, the activity seen within the fusion should decrease in size and intensity. Focal abnormalities within the spinal fusion mass have also been identified in asymptomatic patients, and may represent painless pseudoarthrosis. Late pseudoarthrosis (over 4 years old) may not demonstrate increased tracer localization and this may be related to decreased osteoblastic activity. These lesions, although present, may not be clinically significant as they do not alter skeletal metabolic activity. Asymmetric SI joint activity is also noted frequently in patients that have undergone spinal fusion (up to 75% of cases), with the side of the bone graft harvesting showing less activity than the contralateral side. Increase SI joint uptake can also be seen and may be related to alterations in spinal mechanics [1]. Scintigraphy has a sensitivity of 78% and a specificity of 83% in the detection of pseudoarthrosis, which is superior to plain radiography (43% and 50%, respectively). [1-5]
Bone
Grafts:
Bone scintigraphy can also be used to evaluate whether a bone graft is viable or non-viable. Vascular patency to the graft is characterized by normal or diffusely increased tracer uptake throughout the graft. Focally increased uptake may be seen at the osteotomy sites. When grafts have lost their vascularity they do not concentrate tracer and will appear as photon deficient areas on delayed bone images with reduced flow on the perfusion study. It is important to remember that the scan is most useful for predicting vascular patency and osseous metabolic activity ONLY when the scan is performed within one week of surgery. Scans performed later may be incorrectly interpreted as showing graft viability because of "periosteal creep" (i.e.: new bone deposition on a non-viable graft). Additionally, although tracer uptake is equated with graft viability, this finding has also been described in patients with osteoradionecrosis- a serious complication of radiotherapy for head and neck tumors. Consequently, the presence of increased uptake in patients who have undergone radiotherapy after mandibular reconstruction cannot be automatically equated with graft viability [1].
Joint Prosthesis Imaging:
The are two forms of hip prostheses- a total hip arthroplasty (THR) which consists of femoral head and shaft components; and a resurfacing arthroplasty (RA) in which the native femoral neck is preserved [23]. The recommended range for the acetabular cup inclination is 35-55 degrees and for cup anterversion 10-30 degrees [23]. A vertically oriented cup may result in excessive loading at the edge of the acetabular cup [23].For a THR, the femoral stem should be placed in an anatomic position [23]. For a RA, the position of the resurfacing femoral stem should be central in the femoral neck on the frontal view (the position seen on the lateral view is thought to be less critical, but the pin should not impinge on the cortex) [23]. Occasionally there is notching of the superior femoral neck that is likely related to surgical trauma [23].
Lucency around the component or migration of the component are signs of loosening [23].
A metal induced ractive mass (aseptic lymphocyte dominanted vascular associated lesion) can develop due to a hypersensitivity reaction to metal particles that have been shed from the prosthesis [23]. These reactive lesions can be predominently solid [23]. Risk factors for developing a reactive mass include female sex (8:1 greater risk than men), small prosthetic cup size, poor positioning of the components, and inadvertant downsizing of the femoral head in women with high preoperative head-neck diameter ratios [23]. Presening symptoms are often delayed and include pain, a palpable mass, and femoral neuropathy [23]. The incidence of reactive mass is variable and depends on the type of prosthesis used, but can be up to 8% of large femoral head metal-on-metal THR's [23]. Patients with bilateral RA who develop a reactive mass in one hip, have a 33% chance of having a lesion on the other side [23].
The masses can be identified on US, CT, and MR [23]. The lesions may have a variety of appearances and appear either cystic or solid [23]. Predominently solid lesions tend to be located anteriroly, usually within the psoas muscle and may extend into the pelvis [23].Predominantly cystic lesions tend to arise from the posterior joint space [23]. Lateral lesions tend to involve the trochanteric bursa [23].
Prostheses are fixed to bone to prevent unwanted movement [26]. The componenets can be fixed to bone with, or without cement [26].
Cemented prostheses are anchored in position with polymethylmethacrylate which fills the spaces between the bone and the prosthesis- this creates a "mantle" around the prosthesis that produices a uniform fit with evenly distributed forces [26]. Tracer uptake on bone scan at the distal tip of the prosthesis is not commonly seen (only about 10% of patients). If identified, it is typically mild. Activity greater than the intensity of the iliac crest seen only on delayed images (i.e.: normal flow and blood pool) is strongly indicative of loosening. If the uptake about the acetabular component of the prosthesis exceeds that of the activity of the iliac crest, this is also indicative of loosening.
Uncemented components rely on a tight or
"presed" fit into bone for initial fixation [26]. Cementless
prostheses become fixed via
bony
in-growth into a textured or porous coating applied to the surface of
the
prosthesis (permanent fixation is achieved via the ingrowth of
trabelcular bone over 4-6 weeks) [26].
Normal plain film findings:
The normal acetabular cup has approximately 40? of lateral
inclination (ie: superior tilt relative to a horizontal line, such as
between the ischial tuberosities) and 15? of anteversion [26].
Normal scintigraphic findings:
Oswald et al. reported on the bone scan findings in uncomplicated porous coated hip arthroplasties [6]. Increased blood flow or focal blood pool abnormality are only rarely seen in uncomplicated prostheses. Diffusely increased blood pool activity within the muscle groups of the ipsilateral leg is seen in up to 40% of patients at some time during their post-operative course and can be seen as late as 24 months post operatively. This may be related to increase muscle usage in patients who were previously less active. Delayed activity at the distal tip of the prosthesis can be seen in all porous prosthesis at some time. Even 2 years post-op, activity could still be identified medially (15%), distally (70%), and laterally (50%). Activity in the medial segment was always less than or equal to lateral segment activity. Analysis of intensity over time demonstrated a clear trend toward stable or decreasing activity within the medial segment. Although this trend is generally observed in the distal and lateral segments as well, activity in these areas may also be noted to increase over time. This activity was not indicative of prosthetic loosening. Increased tracer activity can also be identified about the acetabular component of the prosthesis (present in up to 76% of patients even after two years) [13]. In uncomplicated prostheses, acetabular activity generally remains stable or decreases in intensity over time [13].
Persistently increased uptake of Tc-MDP in heterotopic bone occurs in most patients with hip prostheses. This is in contradistinction to Tc-MDP uptake in heterotopic bone in paraplegic patients which decreases as the bone matures.
Infection is a serious complication of joint replacement and can occur in 1% to 4% of patients for hip prostheses (the rate of infection following revision surgery is somewhat higher [15,17]). About one-third of infections develop within 3 months, another third within one year, and the remainder develop more than 1 year after surgery [15]. Staphylococcus epidermidis and S aureus are the most common organisms [15]. Patients often present with joint pain that can also occur in patients with aseptic loosening. Nonspecific markers of inflammation such as the ESR and c-reactive protein may also be elevated in both infection and aseptic loosening [19]. Aseptic loosening is believed to be cased by repeated mechanical stress and local host response to the wear debris of high-denisty polyethylene, metals, and bone cement [21]. An infected joint prostheses requires a resection arthroplasty, a long course (several weeks) of antibiotics, and a lengthy hospitalization. Revision arthoplasty is then performed several months later [17]. Differentiation of aseptic loosening from infection is therefore vitally important [15]. Joint aspiration suffers from large numbers of false positive (3-16%) and false negative (up to 10%) results [15,22]. Plain film findings are usually normal (50%) in patients with septic hip prosthesis. Non-focal periprosthetic bone resorption more than 2mm wide is non-specific and can also be seen in loosening.
Conventional bone scintigraphy has a sensitivity of 65%, specificity of 70%, and an accuracy of 50-70% [15] for the diagnosis of infected prosthesis. Oswald et al. reported on the bone scan findings in uncomplicated porous coated hip arthroplasties [19]. Even in patients without loosening or infection, increased tracer activity can seen about the distal tip at 2 years medially (15%), distally (70%), and laterally (50%). With infection, classically, the bone scan is 3-phase positive with diffusely increased periprosthetic activity on delayed images associated with infection (as opposed to loosening in which there is a focal abnormality identified about the prosthesis) [15,17]. The appearance is probably due to generalized osteolysis. Unfortunately, the findings on bone scan are non-specific and there is considerable overlap between infection and loosening [15]. False positive scans can occur due to dystrophic ossification, periprosthetic granulomas, the altered distribution of red marrow, aseptic loosening, damage of the polyethylene surface of the prosthesis, and metallosis. None-the-less, bone scintigraphy is useful as a screening test because a normal scan essentially excludes a prosthetic complication [15].
Labeled WBC imaging can also be used to evaluate for the presence of an infected prosthesis. WBC imaging should be most useful in detecting leukocyte mediated infectious processes- such as an infected prosthesis- and uptake should be absent in loosening (in which the associated inflammatory reaction lacks significant leukocytes) [17]. On average, combined In-111 WBC-bone scintigraphy imaging has a sensitivity of about 67%, and a specificity of 78% for the detection of prosthetic infection. Note that the patients white blood cell count does not correlate with the amount of In-111 WBC uptake and that the patient may have a normal WBC count, even with an infected prosthesis.
Normal post operative In-111 WBC scan findings have been described prior to the use of combined bone marrow scintigraphy and the findings were likely related to bone marrow activity. In-111-WBC uptake was described at the prosthesis tip in 80% of patients at some time, and still present 2 years post-operatively in 50% of patients. Two distinct patterns of WBC uptake were seen identified: Focal (55%) or diffuse linear (45%) activity within the marrow space below the tip of the prosthesis. This uptake demonstrated a clear trend toward becoming stable or decreasing over time in 90% of patients. In 111-WBC activity was also usually less than (32-60%) or equal to (17%) the activity within the iliac crest. Abnormalities with activity greater than that in the iliac crest should be considered suspicious for infection. In comparison to the Tc-MDP scan, the intensity of In 111-WBC uptake at the tip of the prosthesis was less than or equal to the Tc-MDP uptake in 85% of patients (using the iliac crest as a reference). In-111 WBC accumulation also occurs about the acetabular component of the uncomplicated prosthesis in up to 92% of cases and can still be seen even after two years [13]. The activity is always less intense or equal to activity in the iliac crest and typically remains stable or decreases in intensity over time [13]. Mild WBC accumulation can be seen within heterotopic bone and this should not be confused with the presence of infection. Inguinal nodal activity may also be seen- the lateral view is helpful in demonstrating that the abnormality is anterior to the hip. Additionally, patients with heterotopic bone or inguinal nodal activity typically do not demonstrate a flow or blood pool abnormality on their bone scan.
Presently, evaluation of a suspected infected joint prosthesis is best accomplished by combined In-111 WBC- Tc99m sulfur colloid scintigraphy [20]. Localized ectopic bone marrow expansion may occur in the appendicular skeleton after trauma (fracture), surgical interventions- such as joint prosthesis surgery, neuropathic joint, inflammation, or even calvarial hyperostosis [16,20]. Combined leukocyte-marrow imaging can overcome many of the problems created by variable marrow distribution post-operatively and should be used regularly. In leukocyte imaging it is neither the presence nor the intensity of labeled leukocyte activity, but rather the relationship of such uptake to bone marrow activity that is important [15]. Non-specific In-111 WBC accumulation within areas of ectopic bone marrow can be misinterpreted as infection [15]. The addition of Tc-sulfur colloid (Tc-SC) imaging can aid in evaluation of suspected prostetic hip infection by demonstrating normal bone marrow distribution. Any spatially incongruent area of In-111 WBC tracer activity which does not match marrow activity should be considered consistent with infection (regardless of the intensity of the tracer uptake) [15]. When the distributions of the two tracers are spatial congruent, the exam is negative for infection [15]. The intensity of WBC uptake can be misleading, even mild uptake is consistent with infection if it is spatially incongruent with marrow activity. Combined marrow scintigraphy using In-111 WBC's and Tc-sulfur colloid provides the best results for the evaluation of the suspected infected prosthesis with sensitivity, specificity, and accuracy greater than 90% [1,15,17,18,20].
For the exam, In-111 WBC imaging are acquired 24 hours following tracer administration [20]. For the bone marrow exam, patients should be injected with 10 mCi of freshly prepared Tc-SC not more than 2 hours old (older agent may result in persistent blood pool and urinary bladder activity that degrade image quality [20]. The interval between injection and imaging shouild be at least 30 minutes to maximize tracer clearance from the circulation [20]. Simultaneous dual isotope imaging is performed using a medium energy parallel hole collimator with a 10% energy window centered on 140 keV for technetium; and a 5% window centered on 174 keV, and a 15% window centered on 247 keV for In-111 imaging [20]. Images should be acquired for 10 minutes per view with a 128 x 128 matrix [20].
|
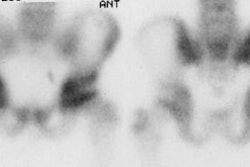
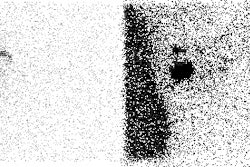
Infected hip prosthesis: The patient shown below underwent evaluation for infected right hip prosthesis using combined In-111 WBC and Tc-sulfur colloid marrow imaging. The white blood cell exam demonstrated incongruent WBC accumulation along the mid and distal portions of the prosthesis (black arrows). Note that other areas of white blood cell accumulation are congruent with the bone marrow scan. The patient had an infected right hip prosthesis. |
|
|

Sequential bone-gallium imaging can also be used to evaluate for prosthesis infection, but the overall accuracy (70-80%) is less than that of combined In-111 WBC - Tc-Marrow scintigraphy [15,17]. For the gallium exam, the study is negative for infection when the gallium scan is normal, regardless of the bone scan findings, or when the spatial distributions of the two tracers are congruent and the intensity of gallium uptake is less than that of the bone tracer [15]. The exam is positive for infection when the distribution of the tow tracers are spatial incongruent or when their distributions are spatial congruent, but the intensity of gallium uptake exceeds that of the bone agent [15]. The images are equivocal for infection when the distributions of the two tracers are spatial congruent and the intensity of uptakes are similar [15].
FDG PET imaging is also being studied for the evaluation of prosthesis infection.
Hip
Prosthesis Loosening:
By 10 years after implantation, 50% of prostheses demonstrate radiographic evidence of loosening and 30% require revision [15,17]. Aseptic loosening can be treated with a single-stage revision arthoplasty requiring only one hospital admission [15,17].
Loosening
is being increasingly recognized as the result of an immune reaction
(type IV hypersensitivity) between the patient and
the prosthesis [17]. Particulate debris produced by component
fragmentation
activates tissue phagocytes, but the debris is resistant to enzymatic
destruction [17]. Continued attempts to phagocytize
the debris results in bony osteolysis and
loosening
[17]. Histopathologically, a pseudomembranous
structure develops in the soft tissues at the bone-prosthesis interface
containing mostly histiocytes, giant
cells, lymphocytes, and
plasma cells
[17]. Neutrophils are present in less than
10% of the
cases (unlike in infection in which neutrophils
predominate) [17]. Aseptic lymphocytic vasculitis-associated lesion
(ALVAL) is the name that is now commonly applied to the condition [25].
It has also be referred to as aggressive granulomatosis
or
granulomatous
pseudotumor). ALVAL is particularly
associated with metal-on-metal total hip replacements
and can be associated with a poor outcome following revision surgery in
patients with advanced disease [24].
Plain film findings which support porous prosthesis loosening include finding a lucent line wider than 2mm adjacent to 3 of the 7 regions about the prosthesis. These findings are felt to represent mechanical loosening. Serial plain film radiographs have sensitivities of 95% and 100% for the detection of loosening of the acetabular and femoral components (respectively) [14].
Unlike aseptic osteolysis, which can be identified as a zone of lucency around the prosthesis, plain films are generally of limited value for the detection of aseptic lymphocytic vasculitis-associated lesion as the films are usually normal [24]. ALVAL can appear as an area of radiolucency/resorption of the medial calcar adjacent to the prosthesis [24], that does not conform to the shape of the prosthesis and can progress over time. Both of these findings, however, have also been described in association with infection.
On bone scintigraphy, focal
abnormalities (not diffuse) in two or more zones or intense uptake in
one zone
about the prosthesis is indicative of loosening [14]. For acetabular loosening, the sensitivity of bone
scanning is
97%, and the specificity is 95% (Accuracy 90%) [14]. For
femoral component loosening the bone scan sensitivity is 85%, and the
specificity 100% (Accuracy 89%) [14]. Therefore, bone scan does not
always
provide additional information with regard to loosening of the hip arthroplasty compared to serial plain film
evaluation [14].
Bone scan is probably most useful when the radiographs are inconclusive
with
regard to loosening [14]. In aseptic loosening there is an associated
inflammatory infiltrate consisting of predominantly lymphocytes and
giant cells
(neutrophils are usually not present in
significant
numbers). As such, gallium scintigraphy
can
demonstrate increased uptake in aseptic loosening which may be
misinterpreted
as infection. In-111 WBC imaging should not be positive with aseptic
loosening
due to the absence of leukocytes. In general, if the plain radiographs
do not
show loosening, an aspiration of the hip is negative, and there is no
increased
activity on a bone scan, then the hip arthroplasty
is
neither loose nor infected [14].
MRI with metal artifact reduction sequences can be used to identify
ALVAL [24]. Since magnetic susceptabiloity artifact is directly
proportional to field strength, the use of high-field strength systems
should be avoided [24]. The main finding on MRI is a periprosthetic
soft-tissue mass or fluid collection with a thick, ragged capsule
characteristically extending from the from the neck of the femoral
component [24].
The incidence of infection after TKA has ranged from 1 to 2% [7,15]. The risk for infection following revision is slightly higher (about 5%) [19]. Aspiration of the knee is helpful, but negative results do not exclude a deep infection [7]. It is even more difficult to assess total knee replacements on bone scan, because 60% of the femoral components and 90% of the tibial components demonstrate increased periprosthetic activity more than 1 year after surgery in asymptomatic patients [1,8]. Periprosthetic activity can persist for several years [17].
White blood cell imaging has a sensitivity, specificity, and accuracy of approximately 85% in the diagnosis of infected knee prosthesis [7]. False positive exams have been reported in association with active rheumatoid arthritis and with massive osteolysis of the adjacent femur and tibia [7].
|
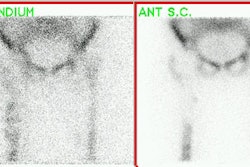
Infected knee prosthesis: The patient had a history of an infected right knee prosthesis. Combined In-111 WBC and Tc-sulfur colloid marrow imaging was performed to evaluate for residual infection following treatment prior to re-do knee replacement. The white blood cell exam demonstrated incongruent WBC accumulation along the mid portion of the right knee joint (black arrow) consistent with unresolved infection. |
|
|


REFERENCES:
(1) Semin Nucl Med 1995; Palestro CJ. Radionuclide imaging after skeletal interventional procedures. 25: 3-14
(2) J Nucl Med 1993; Collier BD, et al. Bone scintigraphy: Part 2. Orthopedic bone scanning. 34(12):2241-6. Review.
(3) J Nucl Med 1989; Lusins JO, et al. Bone SPECT in patients with persistent back pain after lumbar spine surgery. 30: 490-96
(4) J Nucl Med 1994; Even-Sapir E, et al. Assessment of painful late effects of lumbar spinal fusion with SPECT. 35(3):416-22.
(5) Skeletal Radiol 1987; Slizofski WJ, et al. Painful pseudarthrosis following lumbar spinal fusion: detection by combined SPECT and planar bone scintigraphy. 16(2):136-41
(6) J Nucl Med 1989; Oswald SJ, et al. Three-phase bone scan and indium white blood cell scintigraphy following porous coated hip arthroplasty: a prospective study of the prosthetic tip. 30(8):1321-31.
(7) Clinical Orthopaedics and Related Research 1990; Rand JA, Brown ML. The value of indium 111 leukocyte scanning in the evaluaiton of painful or infected total knee arthroplasties. 259: 179-182
(8) Nuclear Medicine Annual 1994, Palestro CJ. Musculoskeletal infection. Ed. Freeman LM. Raven Press, Ltd. New York. 91-119
(9) Radiology 1988; Magnuson JE, et al. In-111-labeled leukocyte scintigraphy in suspected orthopedic prosthesis infection: Comparison with other imaging modalities. 168: 235-239
(10) British Journal of Radiology1992; Miles BKA, et al. Scintigraphic abnormalities in patients with painful hip replacements treated conservatively. 65: 491-494
(11) British Journal of Radiology1992; Copping BC. The role of 99m-Tc-HMPAO white cell imaging in suspected orthopaedic infection. 65: 309-312
(13) J Nucl Med 1990; Oswald SG, et al. The acetabulum: A prospective study of three-phase bone and indium white blood cell scintigraphy following porous-coated hip arthroplasty. 31: 274-280
(14) J Bone Joint Surg [Br] 1993; Lieberman JR, et al. Evaluation of painful hip arthroplasties. Are technetium scans necessary? 75-B: 475-78
(15) Radiographics 2001; Love C, et al. Role of nuclear medicine in diagnosis of the infected joint replacement. 21: 122901238
(16) J Nucl Med 1998; Kaim A, et al. Ectopic hematopoietic bone marrow in the appendicular skeleton after trauma. 39: 1980-1983
(17) J Nucl Med 2003; Palestro CJ. Nuclear medicine, the painful prosthetic joint, and orthopedic infection. 44: 927-929
(18) J Nucl Med 2004; Pelosi E, et al. 99mTc-HMPAO-leukocyte scintigraphy in patients with symptomatic total hip or knee arthroplasty: improved diagnostic accuracy by means of semiquantitative evaluation. 45: 438-444
(19) J Nucl Med 2004; Love C, et al. Diagnosing infection in the failed joint replacement: a comparison of coincidence detection 18F- FDG and 111In-labeled leukocyte/ 99mTc-sulfur colloid marrow imaging. 45: 1864-1871
(20) Radiographics 2006; Palestro CJ, et al. Combined labeled leukocyte and technetium 99m sulfur colloid bone marrow imaging for diagnosing musculoskeltal infection. 26: 859-870
(21) J Nucl Med 2009; Lorberboym M, et al. The use of 99mTc-recombinant human annexin V imaging for differential diagnosis of aseptic loosening and low-grade infection in hip and knee prosthesis. 50: 534-537
(22) AJR 2011; Squire MW, et al. Preoperative diagnosis of periprosthetic joint infection: role of
aspiration. 196:
875-879
(23) AJR 2011; Ostlere S. How to image metal-on-metal prostheses and
their complications. 197: 558-567
(24) AJR 2012; Yanny S, et al. MRI of aseptic lymphocytic
vasculitis-associated lesions in metal-on-metal hip replacements. 198:
1394-1402
(25) Am J Clin Pathol 2010; Watters TS, et al. Aseptic
lymphocyte-dominated vasculitis associated lesion: a clinicopathologic
review of an unrecognized cause of prosthetic failure. 134: 886-893
(26) Radiographics 2012; Roth TD, et al. CT of the hip prosthesis:
appearance of components, fixation, and complicaitons. 32: 1089-1107