Aortic Aneurysm:
View images of aortic aneurysm
Clinical:
The ascending aorta extends from the aortic root to the origin of the right innominate (brachiocephalic) artery [17,19]. The aortic root is defined as the part of the ascending aorta that contains the aortic valve, annulus, and sinuses [17]. The aortic arch extends from the right brachiocephalic artery to the attachement of the ligamentum arteriosum [17]. From the ligamentum arteriosum to the diaphragmatic hiatus is the decending thoracic aorta [17]. Aortic aneurysms can be classified as either fusiform or saccular (a focal out-pouching of the wall). The normal diameter of the mid-ascending aorta should always be less than 4 cm, and that of the descending aorta no more than 3 cm [17]. The risk of rupture increases with the size of the aneurysm [17,19] and there is an increased risk for rupture when the aneurysm is greater than 5 cm in diameter
Abdominal aortic aneurysms expand at a rate of 2-4 mm per year when smaller than 4 cm, 2-5 mm per year when they are between 4-5 cm, and 3-7 mm per year when larger than 5 cm [9]. The risk for rupture of an abdominal aortic aneurysm is between 10-20% when it reaches 5-6 cm, and increases to 30-50% when it equals or exceeds 8 cm [19]. Although thoracic aortic aneurysms expand at a slower rate than abdominal aortic aneurysms, surgical repair is contemplated when the aneurysm reaches a diameter of 5-6 cm (and for descending thoracic aneurysms greater than 6.5 cm) [17]. An annual growth rate of greater than 1cm [17] or a diameter greater than 4.5 cm with an increase of at least 0.5 cm in the preceding 6 months are other accepted indications for surgical repair [17,19]. Earlier intervention is recommended in patients with Marfans syndrome (aortic diameter of 5 cm) [17]. A hyperattenuating cresentic rim if seen on CT of a large abdominal aortic aneurysm is a specific sign of impending rupture [18].
The mortality rate for elective surgical repair of thoracic aortic aneurysms can be as high as 7-12% [15]. The two most common techniques for surgical repair are interposition graft and inclusion graft [17]. After the affected segment has been excised, an interposition graft is sewn end-to-end and vascular branches such as the coronary arteries are reimplanted [17]. An inclusion graft is inserted into the aortic lumen, leaving a potential space between the native aorta and the graft that may thrombose (or even show persistent blood flow that would not require intervention in the absence of hemodynamic instability) [17].
Prior to surgical repair of ascending thoracic aortic aneurysms it is important to document if the aneurysm involves the aortic arch or extends to the inominant artery. In such cases hypothermic circulatory arrest will be necessary for the procedure. This entails cooling the patient systemically to below 19 degrees Celsius, placing the patient in the Trandelenburg position, and stopping the cardiopulmonary bypass circuit. Hypothermic circulatory arrest increases the complexity, length, and mortality associated with surgery. It is also used for some patients with severe aortic calcification where clamp placement leads to an increased risk for stroke due to thromboembolic phenomena, in patients with fragile aortic tissue (Marfan's) where clamping may result in aortic laceration, and in patients undergoing repeat aortic surgery [1].
Etiologies for thoracic aortic aneurysms include:
1- Atherosclerotic vascular disease:
Atherosclerosis is the cause of about 70% of all thoracic aortic aneurysms [17]. Atherosclerotic aneurysms can involve any portion of the thoracic aorta, but most commonly descending thoracic aorta [17] and typically produce a fusiform enlargement involving a long segment of the vessel. About 28% of patients with thoracic aortic aneurysms will also have an AAA [17]. Atherosclerotic aneurysms of the ascending aorta typically spare the sinotubular junction and aortic valve function until late in the disease process. Most thoracic aortic aneurysms are asymptomatic. When symptoms do occur, they are typically related to rupture, dissection, or compression of adjacent structures. The treatment for descending thoracic aortic aneurysms is surgical resection and replacement with prosthetic graft. Mortality rates of up to 50% have been reported in cases of emergent repair, and about 12% in elective cases. Paraplegia occurs in 5-10% of patients. Translumenal endovascular stent grafting offers an alternative method of therapy. The aneurysm must be at least 2-3 cm from the origin of the left subclavian artery to ensure that the stent does not cover the orifice of this vessel. To limit exclusion of intercostal arteries the length should be kept to a minimum. Mortality from the procedure has been reported to be about 15%, and paraplegia occurs in 4% of patients [3].
On MR spin echo images, the wall of the vessel is thickened and irregular secondary to the presence of sclerotic plaque. Areas of signal void correspond to wall calcifications. Thrombus adherent to the wall of the aneurysm may be difficult to distinguish from plaque, although thrombus typically has a smooth interface with the vessel lumen.
2- Marfan's disease / Ehlers-Danlos:
Marfan's syndrome is inhereted as an autosomal dominant disorder with high penetrance, but expression is highly variable. The disorder has been linked to a fibrillin gene defect on chromosome 15 [4].
Both Marfan's and Ehlers-Danlos are associated with cystic medial necrosis that results in weakening of the aortic wall typically resulting in aneurysms of the ascending aorta. Annuloaortic ectasia is characterized by dilated sinuses of Valsalva with effacement of the sinotubular junction producing a pear-shaped aorta that tapers to a normal aortic arch and the condition is most commonly associated with Marfans syndrome [17]. Associated valvular dysfunction is also common secondary to dilatation of the aortic root. Other causes of annuloaortic ectasia include idiopathic (about 1/3'd of cases), homocystinuria, and osteogenesis imperfecta [17].
On MR imaging, there is dilatation of the aortic root associated with complete effacement of the sinotubular junction (remember, this is not seen in atherosclerotic aneurysms until late). When viewed in an oblique coronal section this produces an "onion bulb" or "pear-shaped" appearance to the aortic root and this is considered to be characteristic of the disorders. Cine gradient images can be used to demonstrate regurgitant flow associated with valvular dysfunction.
3- Aortitis:
a) Non-infectious Aortitis: Takayasu's (pulseless disease) and temporal arteritis (giant cell arteritis) are the two most common arteritides to involve the aorta. Takayau's more commonly involves the aorta. Both disorders affect women most commonly- Takayasu's affecting women in their teens to thirties, and temporal arteritis affecting older women. Both aneurysm and stenosis are formation are common. Involvement of the aortic root is also common when there is aneurysmal dilatation and hence, regurge is also seen. The disorders typically produce associated thickening of the aortic wall.
b) Infectious Aortitis (also referred to as Mycotic aneurysm): The most common organisms are Staphylococcus (older males), Streptococcus, Pneumococcus, or Salmonella (younger or immune compromised patients). Etiologies include post-aortic or coronary artery bypass surgery. Prognosis is grim in the absence of antibiotic or surgical treatment. Mycotic aneurysms are usually saccular and contain eccentric thrombus [17]. MR findings indicative of an infectious aortic aneurysm include wall thickening (with or without nodularity), periaortic inflammatory changes resulting in thickening of the periaortic tissues, and a saccular aneurysm (although, fusiform aneurysms can also occur).
Syphilitis aortitis causes focal destruction of the media with loss of elastic and smooth muscle fibers and scarring leading to aortic dilatation and aneurysms [17]. Syphilitic aortitis characteristically involves the ascending aorta (36% of cases) followed by the aortic arch (34% of cases) and usually results in aneurysm formation. Syphilitis aneurysms are at high risk for rupture (up to 40% of cases) [17]. On plain film, "pencil-line" fine calcifications within the wall of the vessel are considered classic.
4- Aortic stenosis:
Post-valvular dilatation of the ascending aorta is seen in association with aortic stenosis. There is relative preservation of the aortic root and sinotubular junction and the dilatation is usually limited to the mid ascending aorta where the post-stenotic flow effects are most pronounced.
5- Aortic insufficiency:
Insufficiency may also result in dilatation of the ascending aorta- likely related to the "water-hammer" effect. Dilatation in these cases is more likely to extend into the transverse arch, and there is less preservation of the aortic root and sinotubular junction.
Endovascular stent grafting:
Endovascular stent grafting is an alternative to surgical repair primary applied to the treatment abdominal aortic aneurysms and for thoracic aortic aneurysms in patients who are poor surgical candidates [15,16]. For asymptomatic patients with thoracic aortic aneurysms, the decision to intervene is complex, but surgery is advocated if the diameter is 5.5 cm or twice the diameter of the normal contiguous aorta [16]. Immediately after endovascular stent placement, CTA imaging may show aortic wall thickening and low density periaortic fluid [16]. Generally, aneurysms will decrease in size following successful endograft repair, however, a slight increase in size of the anuerysm sac may sometimes be seen on the first post-operative scan [16]. As long as no endoleak is identified, conservative management and careful followup can be performed [16]. The left subclavian artery may occasionally be occluded by the stent in order to achieve a minimum of 2 cm length of non-disease aorta for stent anchorage [16]. In these cases, retrograde flow from the left vertebral artery provides perfusion to the left arm [16]. Prior to occlusion of the vessel, cerebral arterial supply should be evaluated to ensure adequate posterior fossa circulation.
For repair of thoracic aortic aneurysms, patients with endovascular stent grafts have been suggested to have a lower prevalence of spinal cord ischemia, a lower prevalence of renal and respiratory insufficiency, and a shorter hospital stay [15]. Patient survival at two years is similar for open repair and stent graft patients [15]. The prevalence of endoleak for thoracic aortic aneurysms has been reported to be 6% at one year, and 9% at two years [15].
Complications of endovascular stent graft include: Endoleaks, stent collapse, stent migration, pseudoaneurysm formation, dissection, aortic perforation, kinking, thrombosis, and coverage of branch vessels [15,16].
1- Endoleak- Endoleak is the most common complication of stent graft repair. An endoleak is defined as blood flow external to the stent-graft and inside the aneurysm sac [13]. Long-term surveillance of patients following stent graft repair of AAA is required as endoleaks can be both and early and late complication of the procedure [14]. Leak can occur in up to 45% of patients (8% to 45% [7]; 15-52% of abdominal aortic aneurysms [12,14]; and up to 29% of thoracic aortic aneurysms [16]). Endoleaks are more consistently identified by multiphasic helical CT than conventional angiography [5,6]. This is because endoleaks have variable flow rates and are often detected at variable times following contrast administration [13]. Typically for the CT evaluation of endoleak, non-contrast, arterial phase, and late-phase images are obtained. Endoleaks seen only on delayed phase images may be more likely to close spontaneously [14].
MR imaging may be superior to CT for the detection of endoleak [11]- however, there are certain limitations to MR. Patients with stainless steel stent grafts should not undergo MR imaging because of the risk of migration or deformation of the graft by the strong magnetic field and extensive artifact associated with this type of stent [13]. Elgiloy stents can also obscure the vessel lumen [13]. Stents composed of nitinol are generally more suited to MR imaging [13].
There are 5 types of endoleaks [7]:
Type 1: The leak occurs at the graft insertion sites (ends of the graft) due to an inadequate seal between the stent graft and the aortic wall. The can be further classified as type Ia (proximal) or type Ib (distal) [13]. These leaks result in elevated sac pressure and a continued risk for rupture. Type I endoleaks are the most common to occur after endovascular repair of thoracic aortic aneurysms (they account for 40% of all endoleaks involving the thoracic aorta) [13,16]. Patients with angulation at the neck of the aneurysm are at an increased risk to develop proximal perigraft endoleaks [14]. These leaks usually appear as broad-based collections directly adjacent to the prosthesis [12]. Large circumferential perigraft collections are indicative of dislocation of the stent-graft or insufficient length a tube endoprothesis [12]. Type I endoleaks are repaired immediately following diagnosis by securing the graft attachment sites with angioplasty balloons, extending the stent coverage with additional stents, or stent graft extensions [13,16,17].
Type 2: The leak occurs when there is retrograde inflow into the aortic sac via a patent branch vessel and it is the most common type of endoleak [10,12,14]. In type IIA endoleaks, there is a single feeding branch vessel, while two or more feeding branch vessels indicate a Type IIB endoleak [16]. For abdominal aortic aneurysms, typical sources include the inferior mesenteric artery and the lumbar arteries [13,14]. For thoracic aneurysms, feeding vessels include bronchial and intercostal arteries, a patent ductus arteriosus, and the subclavian arteries [16]. For abdominal aortic aneuysms- ventral collections without direct connection to the endoprosthesis are supplied by the inferior mesenteric artery, dorsolateral collections are supplied by the lumbar or median sacral artery [13]. Retrograde endoleaks are unavoidable with current endovascular techniques [8]. The risk for type 2 endoleak is increased with increasing patent side branch vessels [7]. The clinical importance of Type 2 endoleaks is not clear. Type II endoleaks (particularly small leaks- less than 15 mm) that have a stable or decreasing aneurysm sac size can be treated conservatively and followed with serial CT evaluation as they have a high rate of spontaneous resolution and a low risk of rupture (more than half of type II endoleaks will spontaneously resolve within the first 6 months) [10,12,13,14]. However, this type of leak (even small leaks) is often associated with failure of the aneurysm to decrease in size and it may actually increase. Treatment should be performed if the feeding vessel is large, if there is significant contrast enhancement in the excluded aortic lumen, or the excluded aortic lumen demonstrates progressive enlargement [16]. Treatment involves embolization of the culprit vessel near its communication with the aneurysm sac to block the retrograde flow of blood [13].
Type 3 occur due to a structural failure of the stent graft including component disconnection, fabric tears/fracture, and disintegration. Junctional dehiscence results from a defect between two adjacent or overlapping stents and often occurs early following technically complex stent procedures [16]. Type III endoleaks are currently fairly unusual, but may become more common during long-term followup [13]. Type 3 endoleaks are treated immediately with a stent graft extension because they represent a direct communication systemic arterial blood with the aneurysm sac [13,17].
Type 4 leaks occur due to transgraft flow due to graft wall porosity. This is an exceedingly rare endoleak and are self limited [12,13]. It is identified at the time of implantation as a blush on the post implant angiogram when patients are fully anticoagulated [13]. These endoleaks require no specific intervention other than normalization of the coagulation profile [13].
Type 5 or "endotension"- no leak is visible radiographically, but the aneurysm continues to grow [5]. Scanning the graft in both the arterial and delayed phases is important to make sure that a subtle leak is not missed.
About 18% of leaks will only be seen on arterial phase images, while about 3% will only be seen on delayed exams. Note that gas may be seen in the aneurysm sac immediately following stent deployment and should not be considered pathologic when scans are performed at that time.
2- Graft thrombosis: Partial, peripheral, or semicirular thrombosis is seen in 3-19% of stents [10]. Graft occlusion is rare [6].
3- Graft kinking: Kinking occurs when large aneurysms shrink/shorten after stent grafting [13]. The kinking may not be detected on transaxial images, but can be demonstrated on MIP or MPR images. Kinking is in turn associated with graft migration, thrombosis, and endoleak [13].
4- Graft migration: Occurs due to poor attachment of the stent to the aortic wall [16]. Migration of 5 mm or more is considered substantial and stent graft position with respect to a constant anatomic landmark should be recorded during followup imaging [13].
5- Shower or peripheral embolism: Shower embolism occurs in 4-17% of cases and is generally fatal [6]. Peripheral embolism can lead to organ or limb ischemia [10].
6- Colonic necrosis (abdominal aortic stent grafting)
7- Aortic dissection (2%) [10].
8- Vascular perforation
9- Pseudoaneurysm associated with graft infection
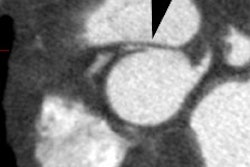
Hx graft repair of an ascending aortic aneurysm: A routine followup CT demonstrated a pseudoaneurysm arising from just above the right coronary artery graft site (black arrows). Surgical repair was performed. There was no evidence for infection. Click image to view cine file- note large amount of low attenuation between graft and native aorta. |
|
10- Stent collapse- predisposing factors are poor stent attachment and oversizing of the stent [16]. On CT there is narrowing of the endolumenal stent diameter and displacement of the stent from the vessel wall [16]. This complication requires urgent surgical intervention when there is significant narrowing of the aortic lumen [16].
REFERENCES:
(2) Magn Reson Imaging Clin N Am 1996; 4(2): 217-235
(3) Society of Thoracic Radiology Annual Meeting Course Syllabus 1997; 21-25
(4) Radiology 1997; 203: 727-732
(5) Radiology 2000; Armerding MD, et al. Aortic aneurysmal disease: Assessment of stent-graft treatment- CT versus conventional angiography. 215: 138-146
(6) Radiographics 2000; Mita T, et al. Complications of endovascular repair for thoracic and abdominal aortic aneurysm: An imaging spectrum. 20: 1263-1278
(7) Radiology 2001; Fan CM, et al. Endovascular stent-graft in abdominal aortic aneurysms: The relationship between patent vessels that arise from the aneurysmal sac and early endoleak. 218: 176-182
(8) Radiology 2001; Gorich J, et al. Endoleaks after endovascular repair of aortic aneurysm: are they predictable?- Initial results. 218: 477-480
(9) AJR 2003; Macura KJ, et al. Pathogenesis in acute aortic syndromes: aortic aneurysm leak and rupture and traumatic aortic transection. 181: 303-307
(10) Radiology 2005; Tolia AJ, et al. Type II endoleaks after endovascular repair of abdominal aortic aneurysms: natural history. 235: 683-686
(11) AJR 2005; Pitton MB, et al. MRI versus helical C or endoleak detection after endovascular aneurysm repair. 185: 1275-1281
(12) Radiology 2006; Chernyak V, et al. Type II endoleak after endoaortic graft implantation: diagnosis with helical CT arteriography. 240: 885-893
(13) Radiology 2007; Stavropoulos SW, Charagundia SR. Imaging techniques for detection and management of endoleaks after endovascular aortic aneurysm repair. 243: 641-655
(14) AJR 2008; Hong C, et al. CLinical significance of endoleak detected on follow-up CT after endovascular repair of abdominal aortic aneurysm. 191: 808-813
(15) Radiographics 2008; Bean MJ, et al. Thoracic aortic stent-grafts: utility of multidetector CT for pre- and postprocedure evaluation. 28: 1835-1851
(16) AJR 2009; Hoang JK, et al. MDCT angiography of thoracic aorta endovascular stent-grafts: pearls and pitfalls. 192: 515-524
(17) Radiographics 2009; Agarwal PP, et al. Multidetector CT of thoracic aortic aneurysms. 29: 537-552
(18) Radiographics 2009; Chao CP, et al. Natural hsitory and CT appearance of aortic intramural hematoma. 29: 791-804
(19) AJR 2009; Litmanovich D, et al. CT and MRI in diseases of the aorta. 193: 928-940