Intravenous contrast enhancement is not the norm in virtual colonoscopy, but it has its place in a growing number of applications, including cancer staging and examination of symptomatic patients.
A study at the 2004 European Congress of Radiology in Vienna aimed to make better use of contrast-enhanced image data by measuring Hounsfield Unit (HU) values in polyps, carcinoma, and the bowel wall. The researchers also hoped to optimize accuracy by relating HU numbers it to specific contrast phases.
"CT value is a function of the contrast phase," said Dr. Wolfgang Luboldt from the Johann Wolfgang Goethe University Hospital in Frankfurt, Germany. "So the purpose of our study was to determine the phase and size related to the tube cutoff for automated mass detection in contrast-enhanced (CT colonography or VC).
Luboldt and colleagues performed contrast-enhanced virtual colonoscopy in 68 patients who had been referred for resection of histologically proven masses, including 27 polyps smaller than 10 mm, 13 polyps 10 mm and larger, and 24 carcinomas.
Following colon cleansing, bowel insufflation and injection of iodinated contrast material, virtual colonoscopy was performed (supine imaging only) in 33 patients, using a four-slice CT scanner at 4 x 1 mm slice thickness, 120 kVp, 100 mAs, 0.5 s rotation speed, 25.5-mm table speed. For an approximate 15 second scan (with the 16-sclice CT), the group used a 60 second delay with 120 ml of iodine and 4 ml/s flow. Five patients were also imaged on a new 16-slice scanner at 16 x 0.75 slice thickness, 120 kVp, 90 mAs (scan delay 70 seconds).
In addition to the HU values of polyps, masses, and the colonic wall, HU values were measured in the aorta (A), the superior mesenteric vein (V), and the height of each mass was measured. Then the HU values of the masses were measured against those of the aorta and superior mesenteric veins using the following formula:
xA+(x-1)V with the value of x varying between 1 and 0.1 (x=0.9, x=0.8...x=0.1).
"The superior mesenteric vein, x, was varied between 1 and 0.1, which means the pure arterial phase," he said. "Zero means portal venous phase."
According to the results, the mean HU of polyps was 150, compared to 108 HU for carcinoma, he said. The best linear correlations were obtained using the following formula from the portal venous phase:
0.4A + 0.6V [r=0.4 (p < 10 mm), 0.77 (p ≥ 10 mm), 0.6 carcinoma]
"To increase the separation between the masses...and the normal colonic wall, the line was shifted (to enable) the highest sensitivity and the highest accuracy," he said.
Thus, at the cutoff line y (A, V) = 0.48067[0.4A+0.6V]-1.235 yielded 92% sensitivity, 86% specificity, 87% positive predictive value, and 92% negative predictive value.
By adding the factor of height using the following formula:
Y (A, V, H) = 1.1023[0.4A + 0.6V]H+69.76
"The accuracy is increased from 89% to 91%" (sensitivity=92%, PPV=92%), Luboldt said, "so the height also affects the cutoff value."
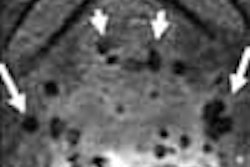
Among the examples was the image of a flat denovo colorectal carcinoma. The cutoff was calculated at 91 HU, and the HU of the mass was 150 -- proof that the lesion was a mass, and not stool or thickened wall, he said.
"Of course, IV contrast is not recommended for asymptomatic persons," Luboldt said, but there are clinical indications like a search for primary cancer, and when you have symptoms, for example, weight loss, anemia, abdominal pain, or if you have a positive pretest, so you can have a secondary screening, in the case of the fecal occult blood test (FOBT)." Staging of tumors and surveillance are other important indications, he said.
Finally, IV contrast can be used without a second procedure if there is residual stool or water, or an obstructing carcinoma that results in an incomplete colonoscopy, Luboldt said.
"IV contrast automates analysis, is faster and perhaps more accurate," he continued. "This test is reader-independent, perhaps company-independent. You can use the information on the HU values as a fourth dimension, and you can superimpose this HU information for automated mass detection," he said.
In conclusion, he said, HU-based segmentation of masses is practicable, and phase-related HU cutoff is more accurate than rigid cutoff values. The correlation to 0.4A+0.6V reflects the weight of the venous phase in contrast-enhanced virtual colonoscopy.
"This formula is a simple approach that indicates a 60-second delay: 30 seconds you have to wait for peak enhancement in the aorta, 10 seconds you have to wait for the transit time (known from previous studies) and you have 20 seconds left for the contrast accumulation," Luboldt said. The 16-slice CT scanner works faster, increasing the optimum delay time to 70 seconds, he added.
By Eric BarnesAuntMinnie.com staff writer
May 24, 2004
Related Reading
Reduced-prep VC with tagging works after failed colonoscopy, April 7, 2004
Experience sharpens role of IV contrast-enhanced VC, January 19, 2004
Copyright © 2004 AuntMinnie.com