Radiographics 2000 Jan-Feb;20(1):59-66
Solitary pulmonary nodules: Part II. Evaluation of the indeterminate nodule.
Erasmus JJ, McAdams HP, Connolly JE.
Department of Radiology, Duke University Medical Center, Durham, NC 27710, USA.
Various strategies may be used to evaluate indeterminate solitary pulmonary
nodules. Growth rate assessment is an important and cost-effective step in the
evaluation of these nodules. Clinical features (eg, patient age, history of
prior malignancy, presenting symptoms, smoking history) can be useful in
suggesting the diagnosis and aiding in management planning. Bayesian analysis
allows more precise determination of the probability of malignancy (pCa).
Decision analysis models suggest that the most cost-effective management
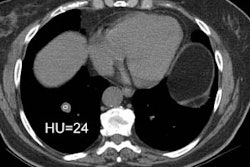
strategy depends on the pCa for a given nodule. At contrast material-enhanced
computed tomography, nodular enhancement of less than 15 HU is strongly
predictive of a benign lesion, whereas enhancement of more than 20 HU typically
indicates malignancy. At 2-[fluorine-18]fluoro-2-deoxy-D-glucose (FDG) positron
emission tomography, lesions with low FDG uptake are typically benign, whereas
those with increased FDG uptake are typically malignant. Results of
transthoracic needle aspiration biopsy influence management in approximately 50%
of cases and, in indeterminate lesions with a pCa between 0.05 and 0.6, is the
best initial diagnostic procedure. It is optimally used in peripheral nodules
and has been reported to establish a benign diagnosis in up to 91% of cases.
Although there is no one correct management approach, the ability to distinguish
benign from malignant solitary pulmonary lesions has improved with the use of
these strategies.