Uterine artery embolization (UAE), an outstanding evolution in women's health in the current century, has become an established noninvasive, safe, and effective alternative to conventional surgical treatment for symptomatic uterine fibroids, the most common gynecological benign tumor.1,2,3,4
UAE was introduced in the United Arab Emirates several years ago in conjunction with ongoing major advancements in the development of healthcare services in general and the expansion of interventional and women's health services in particular.5
Uterine artery embolization
The procedure
There has been increasing global interest in uterine artery embolization as the primary management tool for symptomatic uterine fibroids since the first report in 1995 by Ravina et al.6,7 The principle of UAE is to devascularize the uterine fibroids so as to induce irreversible ischemic injury that leads to necrosis and shrinkage of fibroids.8,9
This is achieved by selective catheterization of both uterine arteries under image guidance and injection of embolization particles.10 Polyvinyl alcohol (PVA) particles are commonly used, but the optimal type and size of the embolization particles is an ongoing debate.11 It is suggested to use particles larger than 300 µm to avoid untargeted ovarian embolization and uterine necrosis.12
 Embolization materials used during a single uterine fibroid embolization procedure at Al Ain Hospital in May 2014. All images courtesy of Dr. Jamal Alkoteesh.
Embolization materials used during a single uterine fibroid embolization procedure at Al Ain Hospital in May 2014. All images courtesy of Dr. Jamal Alkoteesh.Safety and efficacy
The safety and efficacy of uterine artery embolization has been extensively described in the literature. The overall technical success was estimated to be up to 95%.7 Numerous publications have reported not only successful control of symptoms following UAE, but also significant symptom improvement in long-term follow-up when compared to abdominal myomectomy.13,14,15,16,17 Moreover, UAE has a shorter recovery period and minimal blood loss when compared to hysterectomy and myomectomy.7,18
Target population
It is proposed that most women with symptomatic uterine fibroids may be suitable candidates for UAE unless contraindicated.1,19 However, careful individualized assessment of patients by both gynecologists and interventional radiologists remains the cornerstone of decent practice.
Absolute contraindications are current pregnancy, known or suspected gynecological malignancy, and submucosal intracavitary and subserosal pedunculated fibroids which may detach, necessitating surgical intervention.10,20 Conversely, relative contraindications include concurrent gonadotropin-releasing hormone (GnRH) agonist therapy, coagulopathy, severe contrast allergy, renal impairment, immunocompromise, previous pelvic irradiation or surgery, and chronic endometritis or a partially treated pelvic infection.10
Uterine artery embolization in the UAE
Uterine artery embolization was introduced in Abu Dhabi, the capital of UAE, in 2009 by Dr. Jamal Alkoteesh, chairman and chief of interventional radiology at Tawam and Al Ain Hospitals. He has managed within three years to establish one of the busiest fibroid clinics in the Middle East, based at Al Ain Hospital (AAH).
 Team led by Dr. Jamal Alkoteesh at Al Ain Hospital during an embolization procedure.
Team led by Dr. Jamal Alkoteesh at Al Ain Hospital during an embolization procedure.We are performing more than 100 cases per year and receiving referrals from countries in the Gulf Cooperation Council (GCC) and elsewhere in the Middle East. Furthermore, many patients are referring themselves to the AAH fibroid clinic after finding about the procedure through the Internet or their physicians.
The procedure has also been made available in almost all major hospitals in Abu Dhabi. This has led to a major advancement in the quality of health services delivered to female patients in the UAE by Abu Dhabi Health Services (SEHA) hospitals.
All cases are discussed at multidisciplinary team meetings within the gynecology department before the embolization procedures are performed. Many gynecologists in the UAE have started to offer uterine artery embolization as a treatment option to their fibroid patients during consultation and when discussing additional treatment options.
Patient preparation
Patients with symptomatic uterine fibroids are being referred to interventional radiology clinics for further assessment and management plans. Patient details, clinical history, physical examination, and imaging and laboratory results are reviewed. The procedure is explained to all patients and informed consent is obtained. All patients are made aware of what to expect from the procedure, its success rate, the risk of failure, complications, and available alternatives.
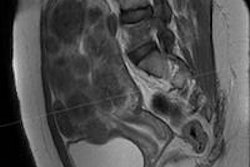
 Bilateral uterine artery embolization for massive uterine fibroids.
Bilateral uterine artery embolization for massive uterine fibroids.Fertility issues
Uterine-sparing therapy is essential in the United Arab Emirates owning to its unique demographics. Most of the country's women are young and unmarried and desire to preserve their fertility. This has made the option of hysterectomy for most of these patients undesirable. On the other hand, there is not yet enough evidence to predict fertility rates after UAE.7
Nevertheless, successful pregnancy outcomes have been reported after the procedure. It has been reported by McLucas et al that the risks of infertility, premature menopause, and hysterectomy after UAE are minor and similar to those associated with abdominal myomectomy.21 In 2010, Narayan et al discovered that the pregnancy success rate following UAE is higher than after abdominal myomectomy.17
Pain management and complications
All patients receive same-day procedures, and they are discharged the same evening. Prompt pain control is achieved by fentanyl patch and nonsteroidal anti-inflammatory drugs (NSAIDs). Patients are closely followed after the procedure to identify any early complications.
UAE complications can occur in 1% to 2% of cases.10 Pelvic pain is the most common complication of the procedure and may last for 48 to 72 hours.22 It should not be taken lightly if pain persists, and conditions such as endometritis, pelvic abscess formation, and endometrial ischemic necrosis should be excluded. Pain associated with fever and nausea is known as postembolization syndrome -- a not uncommon complication -- and is self-limiting within 48 hours. It can be managed conservatively with supportive therapy. Other complications are relatively rare.
Conclusion
Uterine artery embolization is gradually becoming the primary method of treatment for uterine fibroids in the United Arab Emirates. Sparing fertility is a great challenge in the UAE, considering the fact that most of the nation's patients are young, unmarried women. Close follow-up of patients after the procedure is crucial for detecting early complications.
Drs. Jamal Al Deen Alkoteesh, Maysam T. Abu Sa'a, and Haleema P. Saripada are from the department of interventional radiology at Tawam and Al Ain Hospitals in the United Arab Emirates. Correspondence: Dr. Jamal Al Deen Alkoteesh, Al Ain Hospital, email: [email protected], telephone: 00971501029900.
References
- Gonsalves C. Uterine artery embolization for treatment of symptomatic fibroids. Semin Intervent Radiol. 2008;25(4):369-377.
- Bradley LD. Uterine fibroid embolization: a viable alternative to hysterectomy. Am J Obstet Gynecol. 2009;201(2):127-135.
- Pelage JP, Fauconnier A. Uterine fibroid embolization: where are we and where should we go? Ultrasound Obstet Gynecol. 2005;25:527-534.
- Okolo S. Incidence, aetiology, and epidemiology of uterine fibroids. Best Pract Res Clin Obstet Gynaecol. 2008;22(4):571-88.
- Kazmi A. New procedure offers safer alternative to fibroid surgery. GulfNews.com. April 29, 2012. http://gulfnews.com/news/gulf/uae/health/new-procedure-offers-safer-alternative-to-fibroid-surgery-1.1014871. Accessed May 20, 2014.
- Ravina JH, Herbreteau D, Ciraru-Vigneron N, et al. Arterial embolisation to treat uterine myomata. Lancet. 1995;346(8976):671-672.
- Worthington-Kirsch RL. Uterine artery embolization: state of the art. Semin Intervent Radiol. 2004;21(1):37-42.
- Khan AT, Shehmar M, Gupta JK. Uterine fibroids: current perspectives. Int J Womens Health. 2014; 6:95-114.
- Banu NS, Gaze DC, Bruce H, et al. Markers of muscle ischemia, necrosis, and inflammation following uterine artery embolization in the treatment of symptomatic uterine fibroids. Am J Obstet Gynecol. 2007;196(3):213.e1-5.
- Al Shami H, Alkoteesh J. Interventional radiology in obstetrics and gynaecology. Total Radiology. 2013;1.
- Spies JB, Pelage JP. Uterine Artery Embolization and Gynecologic Embolotherapy. Philadelphia: Lippincott Williams & Wilkins; 2005:3-18.
- Worthington-Kirsch RL, Fueredi GA, Goodwin SC, et al. Polyvinyl alcohol particle size for uterine artery embolization. Radiology. 2001;218(2).
- Pron G, Bennett J, Common A, et al. The Ontario Uterine Fibroid Embolization Trial. Part 2. Uterine fibroid reduction and symptom relief after uterine artery embolization for fibroids. Fertil Steril. 2003;79(1):120-127.
- Walker WJ, Pelage JP. Uterine artery embolisation for symptomatic fibroids: clinical results in 400 women with imaging follow up. BJOG. 2002;109:1262-1272.
- Goodwin SC, Spies JB, Worthington-Kirsch R, et al. Uterine artery embolization for treatment of leiomyomata: long-term outcomes from the FIBROID Registry. Obstet Gynecol. 2008;111(1):22-33.
- Spies JB, Ascher SA, Roth AR, et al. Uterine artery embolization for leiomyomata. Obstet Gynecol. 2001;98(1):29-34.
- Narayan A, Lee AS, Kuo GP, et al. Uterine artery embolization versus abdominal myomectomy: a long-term clinical outcome comparison. J Vasc Interv Radiol. 2010; 21(7):1011-1017.
- Smith SJ. Uterine fibroid embolization. Am Fam Physician. 2000;61(12):3601-3607.
- Firouznia K, Ghanaati H, et al. Uterine artery embolization for treatment of symptomatic fibroids: a review of the evidence. Iran Red Crescent Med J. 2013;15(12):e16699.
- Bulman JC, Ascher SM, Spies JB. Current concepts in uterine fibroid embolization. Radiographics. 2012;32(6):1735-1750.
- McLucas B, Goodwin S, Adler L, et al. Pregnancy following uterine fibroid embolization. Int J Gynaecol Obstet. 2001;74(1):1-7.
- Carrillo TC. Uterine artery embolization in the management of symptomatic uterine fibroids: an overview of complications and follow-up. Semin Intervent Radiol. 2008;25(4):378-386.