A new study of Saudi Arabian patients with Middle East respiratory syndrome (MERS) found that a simple method of scoring pathology on lung radiographs can be used to predict which patients are at risk of dying, according to a Web-exclusive article in the American Journal of Roentgenology.
In the study, a multicenter group from hospitals in Saudi Arabia, the U.S., Qatar, and the United Arab Emirates applied a protocol in which three radiologists scored chest radiographs based on the development of MERS lesions over time in a group of 55 patients. They found that the scores correctly predicted which patients would die -- in fact, it was the only factor that showed a statistically significant relationship to mortality, even when conditions such as diabetes mellitus and congestive heart failure were considered.
The researchers believe the scores could be used along with clinical factors to determine which patients should be treated more aggressively (AJR, June 23, 2015, pp. W1-W-8).
A wave of fear
The MERS coronavirus (MERS-CoV) has created a wave of fear and apprehension in the Middle East since the first cases began appearing in 2012; a new outbreak occurred in South Korea in May. The disease is thought to spread to humans from camels, and it has been particularly problematic at healthcare facilities as workers treating MERS patients become infected. About 40% of those infected with the MERS die.
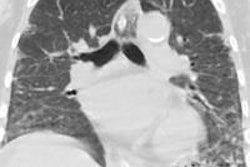
Previous studies have described the unique presentation of MERS on pulmonary CT and radiography exams. But no study has linked the appearance of MERS on imaging studies to the final clinical outcome of patients, according to the research team led by Dr. Karuna Das of King Fahad Medical City in Riyadh, Saudi Arabia.
Das and colleagues decided to explore this question by using a method described by Ooi et al in Respirology (November 2003, Vol. 8:S1, pp. S15-S19) for assessing radiological features of patients with severe acute respiratory syndrome (SARS). Das et al adapted the protocol to score the development of MERS on radiographs of patients who were being treated for the disease.
The first step of the protocol is to divide each lung into three zones, for a total of six zones across both lungs. Then, radiologists assign scores to rate the involvement of disease in each zone, ranging from 0 (normal) to 4 (total involvement of the zone). Finally, the scores are summed to indicate the extent of pathology -- a score of 24 would mean complete involvement of all lung zones with disease.
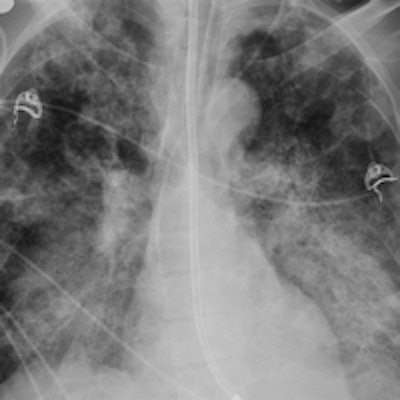
 44-year-old man with end-stage renal disease who developed MERS. Frontal chest radiograph obtained at day 6 shows bilateral multifocal patchy airspace disease with predominant perihilar distribution and multiple areas of cavitation; chest radiographic score is 13. Image courtesy of AJR.
44-year-old man with end-stage renal disease who developed MERS. Frontal chest radiograph obtained at day 6 shows bilateral multifocal patchy airspace disease with predominant perihilar distribution and multiple areas of cavitation; chest radiographic score is 13. Image courtesy of AJR.The protocol was applied in a group of 55 subjects seen at King Fahad Medical City between April and August of 2014; 19 of the individuals ultimately died from MERS and 36 recovered. The study population included 22 healthcare workers, who tended to be younger and have fewer comorbidities than the patients (indeed, only one of the healthcare workers died from MERS, compared with 18 of the 33 patients).
Three radiologists first scored the radiographs at the initial presentation of the subjects, repeating the process at the time of peak radiographic deterioration. They found that the mean score of the subjects who died increased from 1.4 at initial presentation to 13 at the time of peak deterioration (p = 0.001). Death rates were highest in those with the most severe disease progression.
The researchers then compared the radiography scores to other factors that could be used as predictors of mortality for MERS patients, such as the presence of diabetes mellitus, congestive heart failure, and other comorbidities. Radiographic score was the only factor that was statistically significant for predicting mortality, with an adjusted odds ratio of 1.38.
| Factors predicting mortality in MERS patients | ||
| Factor | Adjusted odds ratio | p-value |
| Chest radiographic score | 1.38 | 0.01 |
| Diabetes mellitus | 24.9 | 0.05 |
| Congestive heart failure | 8.41 | 0.16 |
| Absolute lymphocyte count | 1 | 0.96 |
| Age | 0.99 | 0.83 |
| No. of comorbidities | 0.79 | 0.47 |
| Hypertension | 0.47 | 0.61 |
Which radiographic characteristics were most common in the individuals who died? Das and colleagues identified several, including the following:
- Higher incidence of disease involvement in the right lower zone, right middle zone, and left middle zone
- Pleural effusion, pneumothorax, a chest radiographic score of 13 or higher, and worse deterioration, especially when associated with other clinical factors
During the study period, personnel at King Fahad Medical City triaged patients with dyspnea and peripheral ground-glass opacities to a specialized ward for treatment. Nasopharyngeal swabs were performed to test these patients for MERS-CoV infection.
With the results of the current study in hand, Das and colleagues believe that patients who are confirmed to be infected with MERS could be treated more aggressively, particularly those with a radiographic score of 13 or higher, as well as older age and more comorbidities.
"Pleural effusion, pneumothorax, a higher chest radiographic score, and a high number of medical comorbidities in MERS-CoV-infected patients were indicative of a poor prognosis and high short-term mortality," the authors concluded.