Screening asymptomatic patients means justifying the radiation dose, and in recent years virtual colonoscopy practitioners have strived to ramp the dose downward, with an eye on finding the dose levels where noise levels and accuracy might begin to suffer. In Germany, where radiation awareness is keen and many patients ask specifically for dose information, the pressure to keep doses as low as reasonably possible may be even weightier than it is in the U.S.
Dr. Anno Graser and his colleagues from the University of Munich, Grosshadern, wanted to see if adding dedicated z-axis modulation could cut the dose, and if so, to what extent. To do the job they had two 16-slice Sensation 16 scanners (Siemens Medical Solutions, Erlangen, Germany) -- one equipped with online z-axis tube current modulation (Siemens CareDose4D) in addition to x- and y-axis modulation, and the other equipped with the original CareDose software, which works only in the x- and y-axes.
"The purpose of this study was to evaluate the effect of online attenuation-based x-ray tube current modulation of (virtual colonoscopy) in a screening population," Graser said at the 2005 European Congress of Radiology (ECR) in Vienna.
The study included 80 asymptomatic patients, who underwent virtual colonoscopy for polyp screening. The first group of 40 underwent a standard protocol using 120 kVp, with 120 mAs in the supine and 40 mAs in the prone position, with the original CareDose software activated. The second group of 40 patients was scanned with the CareDose4D activated.
"The same (mAs/kVp) values were selected as so-called reference mAs in the CareDose4D protocol -- we need to tell the dose modulation software which values we want to modulate around," he said. "With z-axis tube current modulation, you can only define a reference mAs value, and these were set to exactly the same values."
The tube current modulation tool measured the attenuation automatically during the topogram scan in anteroposterior and lateral dimensions, Graser said. Then the ideal mAs for each table position are calculated in both projection directions, and the mAs level is adapted for each subsequent scan according to the table position. Without modulation, dose varies widely even within the abdomen, he said, overirradiating some areas and underexposing others.
 |
| Even within the abdomen there are large differences in attenuation that can be compensated for by dose modulation in the x-, y-, and z-axes. All charts courtesy of Dr. Anno Graser. |
Image noise was measured subsequently in four regions of interest within the colonic lumen: 1) the porta hepatis, 2) renal hilum, 3) iliac crest, and 4) acetabular roof. Image noise is determined by standard deviation of attenuation (HU) within bowel lumen. "This way we covered the whole scan range, and we have regions of interest at levels with different attenuations," Graser said.
The radiation exposure for each patient was determined by using the dose-length product (DLP) for both the supine and prone scans:
Weighted CTDIvol from scan protocol [mGy] x scan range [cm] = DLP [mGy*cm]
DLP x weighting factors (0.015) = effective dose [mSv]
Dspiral = DCTDIw x effective mAs
Effective tube current-time product [mAseff] = tube current [mA] x rotation time [s]/pitch factor
"This dose-length product times a weighting factor, which we established in a prior study, gives you the effective dose in mSv," Graser explained.
Three independent readers examined endoluminal and MPR views, rating image quality on a 5-point scale (1 being nondiagnostic and 5 being optimal). The cases were displayed in random order without patient data. Finally, a two-tailed student's t-test was used to test for statistically significant differences between the values, and three independent readers evaluated the image quality subjectively on a scale of 1-5.
Graser's results showed that radiation dose was significantly lower in the patient group scanned with CareDose4D (supine position: 4.24 versus 6.55 mSv, p < 0.0001; prone position: 1.61 versus 2.38 mSv, p < 0.0001). The overall radiation dose was reduced by 35% in the supine position and 32% in the prone position, and there was no statistically significant difference in image noise between the four different anatomic levels (porta hepatis: 14.7 [CareDose4D] versus 16.2 HU, p > 0.1; acetabular roof: 28.2 [CareDose4D] versus 29.4 HU, p > 0.30).
 |
| The overall radiation dose and image noise are reduced significantly with the addition of z-axis tube current modulation. |
"The mean attenuation in the lateral projection varies in a stronger way than it does in the anteroposterior dimension," Graser said. "What's happening in the abdomen is that the attenuation in the abdomen (varies) considerably if you were to apply just constant tube current. In the area of the pelvis, you have too little radiation dose, and in the area of the thorax and also in the area of the acetabular roof, you would apply too much radiation dose."
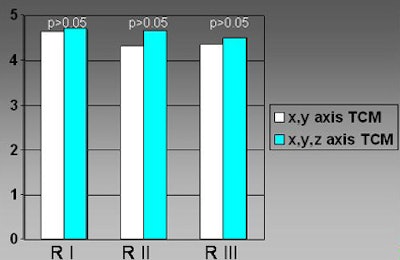
Online attenuation-based z-axis dose modulation led to the significant dose reduction when used in VC, at both the 40 and 120 mAs levels, Graser said. And the three independent readers found no significant differences in image quality between the two protocols, although there was a trend toward better image quality scores in datasets that used z-axis modulation -- especially in the pelvis, where noise tended to be lower, he said.
 |
| Subjective image-quality scores did not significantly improve statistically when z-axis tube current modulation was added, although there was a trend toward better scores using the technique. |
"As you know, dose reduction is especially important in a screening population, where you're screening asymptomatic adults," Graser told AuntMinnie.com. "The background of the whole process is that patients, especially in Germany, are becoming more aware of radiation exposure, and they are explicitly asking us 'What is the radiation dose you are applying in this study?'"
In an earlier discussion of the data, an audience member criticized the group's decision to limit noise measurements to the air of the colonic lumen, rather than including tissue and bone as well. After all, the crucial attenuation difference for polyp detection would be that between polyps and the soft tissue of the colonic wall, he said. In response, Graser explained that initial experiments showed very little attenuation difference between muscle, fat, and air, and as a result, the group decided to limit attenuation calculations to the air in the colonic lumen.
By Eric Barnes
AuntMinnie.com staff writer
April 12, 2005
Related Reading
Diagnostic, screening VC comparable in extracolonic disease detection, December 6, 2004
Ultra-low-dose VC appears feasible, August 3, 2004
Even low-dose VC yields extracolonic findings, September 21, 2004
Copyright © 2005 AuntMinnie.com