A few reports have associated abdominal visceral fat with more aggressive forms of Crohn's disease, but the strength of the association -- and the implications for treatment -- remain unclear. Researchers from Ireland decided to try CT to resolve the issue.
Physicians have many questions about abdominal visceral fat and Crohn's disease: Are patients with more fatty deposits, in fact, sicker? Could physicians use CT depictions of fat deposits to predict disease severity, or could they even target the fat deposits as a potential treatment for severe cases?
Not really, say Irish researchers, who used CT to track abdominal visceral adipose tissue and subcutaneous adipose tissue and match them with Crohn's disease characteristics.
"Patents with longstanding, severe Crohn's disease can suffer severe weight loss, reduced [body mass index (BMI)], and nutritional depletion," said medical student Áine Ní Laoire from University College Cork in Ireland. "Recent research has ... found that visceral fat may be an important component in the inflammatory process. Studies have shown that fibrofatty proliferation around diseased segments of small and large bowel occurs in Crohn's disease."
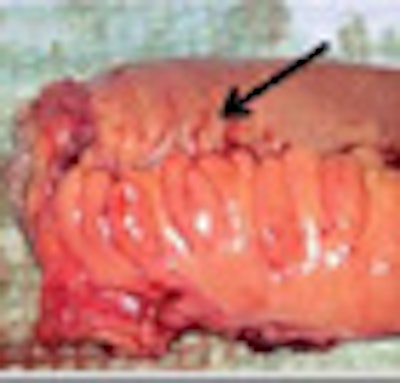
The proliferation of mesenteric adipose tissue (MAT), a metabolically active tissue, produces adipokines, Laoire explained. This so-called MAT hypertrophy, also known as "fat wrapping," is a hallmark of Crohn's disease, and due to its role in the inflammatory process, it is a suggested therapeutic target, she said.
In addition, patients with mesenteric fat hypertrophy have significantly higher clinical and biochemical Crohn's disease activity than patients without mesenteric fat hypertrophy, she said. Visceral adiposity has also been shown to be associated with more severe Crohn's disease progression.
Laoire and colleagues, including Orla Delaney, Sebastian McWilliams, Alan Desmond, and Dr. Michael Maher, aimed to "investigate the association between abdominal adiposity and clinical features of Crohn's disease" using abdominal CT, Laoire said in a presentation at the 2010 European Congress of Radiology (ECR) in Vienna, Austria.
All patients (n = 153, 82 male) had a confirmed diagnosis of Crohn's disease and abdominal CT (n = 276 scans) acquired over the 10-year study period between June 1999 and June 2009. Average measurements were used in the majority of patients who had more than one CT scan.
 |
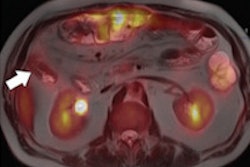
| Fatty regions were isolated and measured based on attenuation of CT images at a single slice (L4/5 intervertebral disk + 6 cm). All images courtesy of Áine Ní Laoire and lead investigator Dr. Michael Maher, University of Cork, Ireland. |
 |
All fat measurements were taken at a single CT slice location (L4/5 intervertebral disk + 6 cm), with investigators measuring visceral adipose tissue area (VAT area, cm2) and subcutaneous adipose tissue area (SAT area, cm2) based on tissue attenuation ranging from -150 to -50 HU. Body mass index was calculated from measurements taken at the L1 level, and CT images were examined using an open-source software package (OsiriX, Geneva), Laoire said. Fifty images were randomly selected for reliability testing using the Bland-Altman method and were found to be acceptable.
SAT and VAT were correlated with patient characteristics including:
- Gender
- BMI
- Smoking status
- Age at diagnosis
- Duration of disease
The two fat types were also correlated with Crohn's disease characteristics including:
- Location (Montreal classification)
- Behavior (Montreal classification)
- Number of surgeries
- Time to initiation of therapy with 6-mercaptopurine (6-MP)
- Time to initiation of therapy with infliximab (IFX)
- Number of IFX infusions
When gender was ignored, patients on 6-mercaptopurine had significantly less SAT overall, while patients on IFX had less VAT/SAT, although with borderline significance, Laoire said. The results also showed a significant positive correlation between age at diagnosis (p < 0.001), duration of disease (p < 0.001), and delay from diagnosis to commencement of 6-MP therapy (p = 0.029) with VAT/SAT ratio.
 |
| When gender was ignored (chart above), patients on 6-MP had significantly less SAT overall, while patients on IFX had less VAT/SAT. Results segregated by gender (chart below) showed significant differences between genders for upper gastrointestinal disease, perianal disease, and IFX use. Significant differences were all found in female patients, and the chart also shows that patients with markers of severe disease have less VAT. |
 |
There were no significant differences in VAT/SAT ratio between disease behavior or location groups.
However, there were significant differences in the mean VAT/SAT ratio for male and female patients in the study (p < 0.001). When analyzing the presence or absence of disease characteristics, significant differences were seen between men and women for upper gastrointestinal disease, perianal disease, and IFX use, Laoire said.
"We found higher visceral adipose tissue in males, and higher subcutaneous adipose tissue in females," Laoire concluded. "When considering females, those with perianal disease and infliximab use had significantly less visceral adipose tissue. However, for males, having markers of severe disease yields no difference in VAT."
"Therefore, we find no evidence that visceral adiposity would be an effective therapeutic target for treating Crohn's disease," she said. "Further studies correlating SAT and VAT with BMI and nutritional indices are necessary to assess the clinical usefulness of this additional information."
In other words, it remains unclear whether the fat is a cause or a consequence of disease severity, Laoire said.
By Eric Barnes
AuntMinnie.com staff writer
April 14, 2010
Related Reading
Nonconstipated IBS patients not at high risk for colonoscopy abnormalities, March 12, 2010
MRI enterography shows shortcomings for Crohn's disease, February 23, 2010
ASIR cuts dose in Crohn's disease patients, December 4, 2009
FDG-PET/CT helps manage treatment for Crohn's disease, November 16, 2009
Colonoscopy findings usually not needed for Crohn's treatment decisions, September 28, 2009
Copyright © 2010 AuntMinnie.com