Correlation was the name of the game in two MR angiography (MRA) studies. A group from New York City looked at whether contrast flow measurements coincided with the severity of peripheral vascular disease (PVD). Meanwhile, Italian radiologists studied whether MR plaque enhancement was in sync with the degree of stenosis in the carotid artery.
Peripheral vascular lesions
For the first study, Dr. Kiyarash Mohajer and colleagues from Weill Medical College of Cornell University evaluated cine phase contrast flow data across stenoses to see if MRA could predict atherosclerotic lesion severity.
"Patients with PVD often have difficulty walking and with progress of disease, they might have pain (during rest), foot ulcers, and ultimately gangrene. Unfortunately, some patients might need (amputation)," explained Mohajer in a talk at the 2005 RSNA meeting in Chicago. "MRA is excellent in showing luminal anatomy, but it is difficult to determine which stenoses can benefit from angioplasty or bypass. In order to know this, we need to know the hemodynamic significance of the lesions."
 |
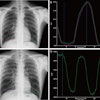
| Normal triphasic flow curves during one cardiac cycle at the level of SFA and popliteal artery. Note the antegrade peak followed by flow reversal and then another lower antegrade peak. This is typical high resistance flow which occurs at rest. |
The group recruited 48 patients who underwent 3D gadolinium-enhanced MRA followed by 2D axial cine phase contrast, above and below the site of greatest superficial femoral artery (SFA) disease severity. Serving as the control group, nine healthy patients underwent imaging on a 1.5-tesla scanner (Signa Excite, GE Healthcare, Chalfont St. Giles, U.K.). In the latter, cine phase contrast flow measurements were obtained at the level of proximal SFA/PFA (profunda femoris artery) and at the level of the popliteal artery.
"We hypothesize that by using 2D cine phase contrast flow measurements, we might be able to see changes across PV (peripheral vascular) lesions that might help us to find the hemodynamic significance," Mohajer said.
 |
| Flow volume curves for right SFA occlusion compared to a left SFA with only mild narrowing. Note in right thigh, loss of triphasic flow and markedly decreased flow volume with SFA occlusion (above). But in the left thigh with only mild SFA disease, triphasic flow is preserved above and below the lesion and there is no peak delay (below). |
 |
The phase contrast data was postprocessed with flow analysis software to obtain flow velocity and flow volume curves above and below the lesion of greatest severity. Two ratios were calculated:
- Peak velocity: flow volume (above/below lesion)
- Incidence of time delay: peak velocity (below lesion)
The pattern of change in the shape of flow curves was observed, and flow parameters were correlated with lesion severity. Mohajer said that obtaining flow measurements took about four minutes while postprocessing required around 15 minutes.
 |
| White lines indicate sites of cine phase contrast flow measurements. |
Results were derived from 96 arterial segments in 48 patients. Of the 96 segments, 26 were normal or mildly stenotic, 35 had moderate to severe stenosis, and 35 were occluded.
"Our results demonstrate that there is a significant difference in peak velocity ratios above/below the level of stenosis compared to normal healthy volunteers," Mohajer said.
 |
| Flow volume curves demonstrate a moderate web-like right SFA stenosis and multiple severe left SFA stenoses. For moderate web-like stenosis, the peak ratio is 1.85, but there is no peak delay and triphasic flow is preserved below the lesion. But for more severe SFA lesions on the left thigh (below), there is an even higher peak ratio, 2.73 and peak delay of about 34 ms. In addition with severe stenoses there is loss of triphasic flow distal to the stenoses. |
 |
The mean peak flow velocity above/below lesion was significantly higher in the segments with severe disease (1.9) or occlusion (1.4) versus normal segments (1.4). In addition, a delay in peak velocity below lesions showed significant positive correlation with lesion severity, the authors stated in their abstract.
The mean flow volume above/below lesions was 3.9 in occluded vessels and 2.3 in normal volunteers. The group found that flow curves tended to change from triphasic to biphasic or monophasic below moderate to severe stenoses (21 of 35) and occlusions (33 of 35).
 |
| White lines indicate sites of cine phase contrast flow volume measurements. |
Mohajer's group concluded that "changes in flow parameters across PV lesions correlates with severity. This may help determine which lesions are hemodynamically significant obviating the need for invasive pressure measurements."
In a secondary arm of this study, the group tested induced hyperemia using systolic thigh compression with a blood pressure cuff inflated for three minutes. They measured flow before, during, and after compression. Once again, they found that arterial flow changes across atherosclerotic lesions correlated with stenosis severity, Mohajer said.
 |
| Above and below, maximum flow velocity curves show peak delay of 39 ms and loss of amplitude bilaterally distal to SFA occlusions. |
 |
An RSNA attendee asked about the reproducibility of flow measurements at rest, which is given to variation depending on the activity level of the patient. Mohajer explained that their patients usually sat for at least 30 minutes before the scan, but such variations will need to be considered in future studies.
Another session attendee suggested that the hyperemia test might be of limited value in certain patients, such as diabetics with calcified arteries.
 |
| White lines indicate sites of cine phase contrast flow velocity measurements. All images courtesy of Dr. Kiyarash Mohajer. |
"We still have to work on ways to induce that hyperemia," Mohajer said "We were thinking of exercising the patients for two to three minutes, but not all patients will tolerate that. With the experience we have with blood pressure cuffs, even diabetic patients could tolerate the compression. Still, I think exercise is a better way to augment that flow if we don't have the (physical) limitation."
Plaque morphology
Information about plaque morphology and plaque composition is crucial to identify unstable plaque, inflammation, and neoangiogenesis, according to Dr. Nicola Flor from the Instituto Policlinico San Donato in Milan. In his 2005 RSNA talk, Flor shared the results of a study that used electronic subtraction for detecting carotid plaque enhancement on contrast-enhanced MRA.
For this research, 46 patients underwent bilateral carotid MRA using a coronal 3D sequence with an automated bolus of 0.1 mmol/kg of Gd-BOPTA. A 3D fast low-angle shot, T1-weighted sequence was used to image carotid bifurcation, two to four minutes after contrast injection.
 |
| Angiographic image of a patient with 55% stenosis of the common carotid artery. |
Electronic subtraction (unenhanced minus enhanced axial images) was performed. Internal carotid stenoses were graded on maximum intensity projection (MIP) and multiplanar reformatted (MPR) coronal images. North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria were applied to judge the percentage of stenosis.
Plaque enhancement was evaluated on axial images by two radiologists in consensus on a four-point scale (0 equaled no enhancement; 3 equaled clear enhancement). They looked at enhanced, unenhanced, and electronic subtraction images.
The results showed that in 92 carotids mild stenosis was found in 29 segments (NASCET 32%), moderate stenosis in 39 (42%), and severe stenosis in 24 (26%). Plaque enhancement was detected in eight of 46 patients and in nine of 92 carotids. The degree of stenosis in these cases was mild (22%), moderate (67%), and severe (11%).
The mean score for plaque enhancement on unenhanced and enhanced images was 1.44. On subtracted images, the mean score was 2.44.
 |
| Above, the unenhanced image. Below, the enhanced image and the MRA showing plaque enhancement, which is more evident after electronic subtraction. All images courtesy of Dr. Francesco Sardanelli. |
 |
 |
"We can say that subtraction imaging is a useful tool to detect plaque enhancement," Flor said. "Plaque enhancement does not seem to correlate with the degree of stenosis as we see a large prevalence of moderate stenosis."
RSNA session moderator Dr. Christoph Zollikofer asked if Flor's group had studied the pathologic significance of high or low enhancement. Flor said that they had not correlated their results with pathology, but he suggested that hyperintensity may indicate the presence of lipids, while hypointensitiy could represent calcium. The presence of plaque enhancement most likely means extravasation, presence of inflammation, or increased permeability, he added.
"Looking at the future, we have to study the correlation between plaque and histopathology, verify the predictive value of plaque enhancement, and define if plaque enhancement can be used as an additional sign (for) changing treatment planning of carotid stenosis of moderate degree," Flor concluded.
By Shalmali Pal
AuntMinnie.com staff writer
March 10, 2006
Related Reading
CT angiography trumps DSA in renal artery stenosis, says ISET speaker, January 26, 2006
High resolution, fast acquisition give 3D MRA edge in abdomen, January 20, 2006
ACC/AHA issue new treatment guidelines for peripheral artery disease, December 7, 2005
Copyright © 2006 AuntMinnie.com