Dynamic chest radiography (DCR) may serve as a useful tool for evaluating acute respiratory failure with wheezing, particularly when conventional diagnostic tests are inconclusive, researchers have reported.
The finding is from a case series in which DCR imaging was acquired at the bedside of four patients using a portable chest x-ray machine, noted lead author Hidemitsu Miyatake, MD, PhD, of Shiga University of Medical Science in Shiga, Japan, and colleagues.
“Dynamic chest radiography may serve as a practical adjunct that increases diagnostic confidence in emergency and critical care settings where rapid, noninvasive functional assessment is desirable,” the group wrote. The study was published November 13 in Radiology Case Reports.
DCR is an emerging low-dose x-ray technique in which images are acquired at up to 15 frames per second over a 10- to 20-second breath-hold or quiet breathing period. The image data are then post-processed on a dedicated workstation to generate functional images, the authors explained.
One practical advantage is that DCR can be performed using a portable x-ray system equipped with dedicated DCR capability, immediately after a standard chest radiograph. If the initial film is inconclusive, an additional 15-second dynamic acquisition can be obtained at the bedside without patient transfer, the researchers added.
To illustrate its potential, Miyatake and colleagues described its use in four patients with wheezing-associated acute respiratory failure from diverse etiologies: presumed asthma exacerbation, tracheobronchomalacia, cardiogenic pulmonary edema, and endotracheal mucus plugging.
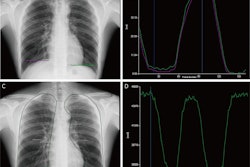
In one case, an 81-year-old woman with no history of asthma developed acute expiratory wheezing and hypoxemia after undergoing transcatheter aortic valve implantation for severe aortic stenosis. A portable chest x-ray showed mild cardiomegaly without overt pulmonary congestion or infiltrates.
Bedside DCR, however, as seen above, revealed increased lung translucency during inspiration, while postprocessing demonstrated reduced pixel-value fluctuations in both lungs, suggesting impaired ventilation and diffuse bronchospasm, the authors wrote. After bronchodilator therapy, the patient’s wheezing and oxygenation improved within one hour.
Based on the clinical course and therapeutic response, the episode was diagnosed as an acute asthma exacerbation, the authors noted.
“Follow-up DCR confirmed recovery of ventilation in both lungs,” they added.
In the three other cases, DCR demonstrated expiratory central airway collapse in tracheobronchomalacia, supported pulmonary congestion without ventilation loss in heart failure, and revealed unilateral ventilation impairment due to mucus plugging in an intubated patient.
Ultimately, DCR is not intended to replace conventional modalities such as radiography, CT, or bronchoscopy, but to contribute supportive dynamic evidence when initial evaluations are inconclusive, the researchers wrote.
“These cases suggest that DCR may serve as a useful adjunct in selected emergency and critical care scenarios when conventional radiography alone is insufficient,” the group concluded.
The full study is available here.