Breast cancer patients often face the additional risk of distant metastases, and the best way to find the presence of those abnormalities in the liver and bone is with PET/MRI, according to a study published in the October issue of Radiology.
Researchers from the New York University (NYU) found that PET/MRI was adept at discovering these abnormalities and exposed patients to half the radiation dose of PET/CT. But the latter modality retained its proficiency in detecting pulmonary metastases.
"In breast cancer patients, PET/MRI can find metastases before PET/CT," said lead author Dr. Amy Melsaether, an assistant professor of radiology at NYU. "We know from other studies that treating those metastases early will improve outcomes for the patients. The next step is finding out for whom this information is most useful."
Detection challenges
Whole-body FDG-PET/CT has long been the modality of choice for diagnosing patients suspected of recurrent or metastatic breast cancer, as well as for evaluating response to therapy. Previous studies have shown that PET/CT can detect distant metastatic disease in 20% of patients with newly diagnosed stage IIb or stage III breast cancer.
 Dr. Amy Melsaether from New York University.
Dr. Amy Melsaether from New York University."With newly diagnosed breast cancer, there is no standard recommendation on how to image the rest of the body," Melsaether told AuntMinie.com. "When breast imaging is done, sometimes unexpected metastatic disease can be present in an estimated 20% of patients, depending on tumor size."
The downside of PET/CT is its low sensitivity for brain and liver metastases and its emission of a relatively high radiation dose, which has potentially adverse effects for young breast cancer patients who face the prospect of multiple periodic scans.
"Early treatment can make a difference in terms of survival and quality of life. So we wanted to see if full-body imaging at the time of diagnosis could detect more metastases," she added. "PET/CT is not performed on all patients; it all depends on tumor size, age of patent, and physician referral. Now we have this new tool -- PET/MRI -- to give us more information."
Imaging protocol
The prospective study included 50 women and one man with breast cancer (mean age of 56 years; range, 32 to 76 years; male age, 70 years) who completed PET/MRI with diffusion-weighted MRI (DWI-MRI) and PET/CT between July 2012 and October 2013. PET/CT scans were scheduled for various reasons, including evaluation after chemotherapy, monitoring distant metastases, and initial staging (Radiology, October 2016, Vol. 281:1, pp. 193-202).
PET/CT scans (Biograph mCT, Siemens Healthineers) were performed approximately 45 minutes after intravenous injection of FDG (mean dose, 547.6 MBq; range, 485 to 566 MBq) from the vertex to the thighs for 24 patients, or from the skull base to the thighs (due to an error in protocol) in 27 patients.
PET/MR images were acquired simultaneously with a PET/MRI scanner at 3 tesla (Biograph mMR, Siemens) a mean of 167 minutes (± 36 minutes) after FDG injection for PET/CT. Scans were conducted from the thighs to the vertex with the patient in the supine position, using a dedicated multichannel head and neck coil and a set of flexible body matrix coils.
Two readers who were blinded to patient histories separately interpreted all PET/CT and PET/MR images. Imaging and clinical follow-up served as the reference standard.
Distant discoveries
Through the scans, the researchers found 242 distant metastatic lesions in 30 patients, 18 breast cancers in 17 patients, and 19 axillary nodes with positive findings in eight patients. Thirteen patients had no evidence of primary or metastatic disease.
In detecting distant metastases in the liver, PET/MRI had greater sensitivity than PET/CT. The researchers credited DWI-MRI in finding up to 40 liver metastases, compared with 28 liver metastases with PET/CT.
| PET/MRI vs. PET/CT for 2 readers | ||||||||
| Sensitivity | Specificity | |||||||
| Reader 1 | Reader 2 | Reader 1 | Reader 2 | |||||
| PET/CT | PET/MRI | PET/CT | PET/MRI | PET/CT | PET/MRI | PET/CT | PET/MRI | |
| Liver | 50% | 78.3% | 88.4% | 99.8% | 94.5% | 92.2% | 100% | 99.9% |
| Lung | 73.5% | 61.5% | 100% | 99.8% | 70.5% | 80.8% | 89.6% | 96.3% |
| Pleura | 73.5% | 73.5% | 100% | 100% | 94.9% | 94.9% | 100% | 100% |
| Distant lymph node | 66.4% | 78.3% | 95.2% | 99.8% | 88.0% | 90.3% | 99.7% | 99.7% |
| Bone | 84.4% | 90.9% | 99.7% | 100% | 90.4% | 92.8% | 99.9% | 100% |
PET/MRI also achieved greater detection of bone lesions, with a combined 207 lesions for both readers, compared with a total of 196 lesions with PET/CT for both readers. In the comparison of lung metastases, both readers tallied a total of 55 true-positive results with PET/CT, compared with 37 true-positive findings with PET/MRI.
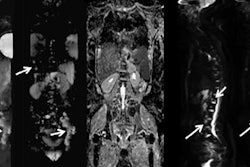
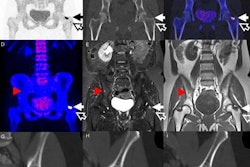
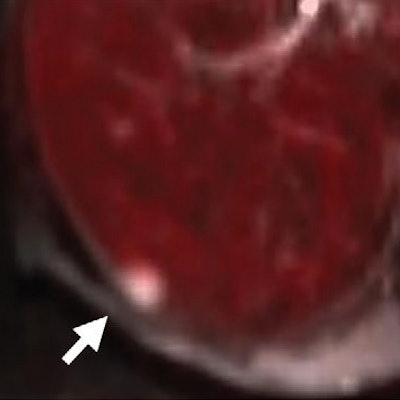
 Axial PET/MRI (a-c) and PET/CT (d) images are from a 64-year-old woman with a history of left breast cancer metastatic to lung and bone. Images were obtained to monitor response during chemotherapy. A liver metastasis (arrow) is seen on PET/MRI (a-c), but not on PET/CT (d). The metastasis is best seen on the diffusion-weighted MR image (a), with corresponding low signal intensity on the apparent diffusion coefficient map (b). There is minimal corresponding FDG uptake on the fused diffusion-weighted and PET image (c). The metastasis is not seen on PET/CT images (d). Images courtesy of Radiology.
Axial PET/MRI (a-c) and PET/CT (d) images are from a 64-year-old woman with a history of left breast cancer metastatic to lung and bone. Images were obtained to monitor response during chemotherapy. A liver metastasis (arrow) is seen on PET/MRI (a-c), but not on PET/CT (d). The metastasis is best seen on the diffusion-weighted MR image (a), with corresponding low signal intensity on the apparent diffusion coefficient map (b). There is minimal corresponding FDG uptake on the fused diffusion-weighted and PET image (c). The metastasis is not seen on PET/CT images (d). Images courtesy of Radiology.In addition, the readers found 15 and 14 brain metastases, respectively, in five (10%) of the 51 subjects with PET/MRI. PET/CT found no brain metastases. The number of brain metastases came as a surprise to Melsaether and colleagues.
"We did not expect that many," she said. "Perhaps we should do more research to see if there are specific types of breast cancer where we would want to perform PET/MRI, such as with HER2 patients who are more likely to have brain metastases."
Radiation reduction
In evaluating radiation levels, CT's effective dose ranged from 2.2 mSv to 16.9 mSv (mean, 8.3 mSv), while PET/CT's effective dose ranged from 11.7 mSv to 26.3 mSv. By comparison, PET's effective radiation dose (which is the same as PET/MRI's effective dose) ranged from 8.2 mSv to 9.9 mSv (mean, 9.3 mSv). Those amounts translate to a reduction range of 19% to 64% and a mean reduction in effective radiation dose of 50% (p = 0.001).
"We think that [50%] makes a big difference for many breast cancer patients who are diagnosed in their 40s and early 50s," Melsaether said. "Radiation exposure is important in younger patients, especially as you monitor them with follow-up exams to make sure there is no recurrence. If these people are treated well, they have many life years left."
There is no standard protocol at NYU when choosing between PET/CT and PET/MRI for breast cancer patients, she added. Physicians order what is most appropriate, but there are some doctors who lean toward PET/MRI over PET/CT.
When to follow-up?
There also are cases when a patient has a negative PET/CT scan, but the physician sees a tumor marker that could indicate the presence of cancer. Those circumstances often lead to a follow-up PET/MRI exam. Melsaether recalled one patient with a negative PET/CT scan, but the subsequent PET/MRI found a liver metastasis. In another instance, a bone metastasis was discovered on follow-up.
"PET/CT at times is a better option, because it is more convenient, it is more of a logistics decision, and it is a quicker exam," she continued. "At NYU, there is only one PET/MRI scanner, whereas we have several PET/CT scanners. We are more set up for PET/CT, which is better at detecting lung metastases, but PET/MRI outperforms PET/CT for brain, liver, and bone metastases, and other surprise primary cancers."
Melsaether and colleagues plan to further refine the current study to determine which patients most benefit most from PET/MRI and its ability to detect distant metastases.
"In most patients, PET/MRI and PET/CT are not prompting a change in treatment," she added. "Even if we see a few more metastases, patients are still being treated."