SPECT myocardial perfusion imaging (MPI) has long been the primary modality for evaluating the extent and severity of coronary artery disease (CAD). But research based on payor data covering millions of patients found that initial evaluation with coronary CT angiography (CTA) instead of SPECT MPI cut costs significantly over a year's time for patients without coronary artery disease and the patient cohort overall.
The use of primary coronary CTA actually pushed costs higher in the subset of patients found to have coronary artery disease, the researchers noted. But they attributed the additional costs to higher rates of revascularization in patients whose coronary artery disease was based on CTA findings, a practice that could presumably improve patient outcomes and cut healthcare costs down the road.
Imaging modalities such as CT and SPECT have enhanced doctors' ability to evaluate suspected coronary artery disease. But the technological advances have also led to marked increases in test utilization, with one-third of all healthcare costs taken up by new technologies.
"The estimated cost of health expenditures in 2007 was $2.3 trillion dollars in 2007, comprising 17% of the [U.S.] gross national product," said Dr. James Min in a presentation at Stanford University's 2008 International Symposium on Multidetector-Row CT in Las Vegas. "Of every healthcare dollar, 8% will be to a physician for imaging services."
Despite the flood of money into imaging, however, opportunity costs associated with the use of one modality over another still aren't well established, said Min, who is an assistant professor of medicine and radiology at Cornell University Medical Center and New York-Presbyterian Hospital in New York City. Costs and outcomes associated with the use of coronary CT as a first-line modality are also unknown.
"We aimed to do a study where we looked at category III tracking codes in a retrospective cohort study to assess the costs and clinical outcomes of coronary CTA," he said.
(Category III codes, also known as tracking codes, are unreimbursed CPT codes used to identify emerging technology and allow data collection for specific new procedures or services in the U.S. The American Medical Association released category III codes for CTA in 2006.)
The study, currently in press, included patients referred for coronary CTA or SPECT MPI between 2005 and 2006. Only patients referred for CTA or SPECT MPI without known coronary artery disease were included.
The database included five large health plans covering more than 6.5 million patients who were enrolled in several different kinds of health plans, including health maintenance organizations (HMOs), preferred provider organizations (PPOs), and Medicare Advantage plans.
The analysis accounted for patient demographics, pharmacy claims, line-item inpatient and outpatient service claims, hospitalization, and procedure and diagnosis codes, Min said.
"From these codes we matched CTA data in 2,300 patients to SPECT data in 9,200 patients," he said. The code utilization analysis for CTA versus SPECT MPI employed a two-level model matched for 11 factors including age (52.9 years), gender (41.5% female), diabetes (10.6%), hypertension (40%), hyperlipidemia (52.5%), peripheral artery disease (1.6%), cerebrovascular disease, cardiac risk score, baseline comorbidity, and type of health plan, Min said.
As calculated by the study team, the care costs included additional testing beyond SPECT MPI or CTA, medical therapies, interventional therapies, and hospitalization related to coronary artery disease, Min said. The researchers also analyzed clinical outcomes including myocardial infarction, angina, CAD-related hospitalization, and outpatient visits. Follow-up costs after the initial test were compared using a generalized linear model with a log link and gamma variance function.
According to the results, CTA patients incurred CAD-related costs that were 26% lower, or $1,075 (95% confidence index [CI], 243, 2,570) less than the cost of SPECT over 12 months of follow-up.
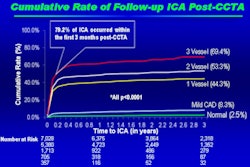
A nine-month resource utilization analysis of coronary CTA versus SPECT MPI showed that in patients with no known coronary disease who underwent coronary CTA, "there was high utilization of downstream nuclear stress testing; whereas in patients who underwent nuclear stress test imaging, there was a high incidence of downstream invasive coronary angiography," Min said. "There was more testing in the CTA arm of the study downstream after the initial test; however, it was with the relatively [less costly] nuclear stress test rather than invasive coronary angiogram."


More patients with coronary artery disease underwent nuclear imaging after CTA (5.3%) compared to SPECT patients (2.3%, p < 0.01), Min said. And more CTA patients (8%) underwent revascularization compared to SPECT patients (5.5%, p < 0.05).
"Patients who underwent CT first were more likely to be successfully revascularized," he said. Coronary CTA patients experienced slightly lower rates of CAD-related hospitalization (1% for CTA versus 2% for SPECT, p = 0.003), as well as lower rates of myocardial infarction or new-onset angina (5% for CTA versus 8% for SPECT, p < 0.0001).

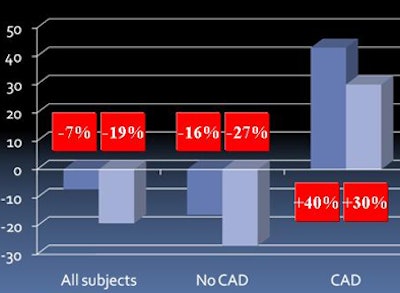
Although CTA cost less than SPECT MPI in the cohort as a whole, it was more expensive, at least initially, in the subset of patients with coronary artery disease.
"Patients who underwent primary CTA without a prior diagnosis of coronary artery disease had a $445 cost savings in a nine-month follow-up period," Min said. "In contrast, patients with coronary artery disease who underwent CTA first had a cost increase of $2,500 compared to patients who underwent nuclear SPECT imaging."
The analysis shouldn't end at that point, however, because CT frequently reveals incidental findings. Could its greater use lead to an increase in downstream non-CAD costs? Not according to the study data, Min said. CTA was less costly for the entire study group and those without CAD, both excluding or including the cost of the initial test.

The researchers also sought to exclude any potential effect of higher utilization resulting from use of the new category III codes. To this end they analyzed the use of CAD-related ICD-9 codes for 2002-2005 in the same database, before the category III codes became available.
The utilization patterns were the same for the old CAD-related category I codes. Coronary CTA patients incurred costs that were 26% ($1,075, 95% CI, 243, 2,570) lower than SPECT during the 12-month follow-up.
"There will be a cost savings in patients who undergo CT in lieu of MPI, and a cost increase in patients with coronary disease," Min concluded. And although there was little difference in clinical outcomes based on the modality used, "CTA patients incurred lower 12-month total CAD-related costs, with slightly lower rates of CAD-related hospitalization, angina, or myocardial infarction diagnosis," he said.
Study limitations included its retrospective design and limited follow-up period. In March of this year, enrollment was completed for a new prospective study of PET, CT, and SPECT, Min said. "We're also designing randomized nuclear [scanning] versus CT for both costs and outcomes," he said.
By Eric Barnes
AuntMinnie.com staff writer
May 30, 2008
Related Reading
Coronary CTA cuts costs for chest pain care, February 29, 2008
ACCURACY trial compares coronary CTA to angiography, January 18, 2008
Coronary CTA study aims for lowest dose, January 11, 2008
Pending Medicare decision roils cardiac CTA, January 8, 2008
Low-dose coronary CTA diagnoses most patients, November 28, 2007
Copyright © 2008 AuntMinnie.com