Use of SPECT/CT can help avoid additional imaging tests for thyroid cancer evaluation and prompt changes in risk classification and treatment management among intermediate- and high-risk patients, according to a study in the September issue of the Journal of Nuclear Medicine.
Researchers at Memorial Sloan-Kettering Cancer Center in New York City also found that SPECT/CT can significantly reduce the number of equivocal findings on post-therapy planar radioiodine-131 (I-131) scans, and the modality provided more accurate characterization of focal iodine accumulation in 20% of patients.
SPECT/CT's enhanced accuracy helped to avoid additional imaging studies in 48% of the patients in the study and prompted a change in risk classification in 6.5% of intermediate- and high-risk patients. The lead author of the study was Ravinder Grewal, MD, from Sloan-Kettering's department of radiology (JNM, September 2010, Vol. 51:9, pp. 1361-1367).
Therapy monitoring
Therapy with I-131 has been an effective way to help determine the extent of thyroid cancer in patients who are believed to be at intermediate to high risk for recurrence of or dying from the disease. Typically, four to seven days after I-131administration, images of the neck, chest, and whole body are taken to detect sites of iodine uptake. Depending on the location, iodine uptake may change a patient's treatment plan. Some patients also may require additional cross-sectional imaging or biopsy for evaluation.
Grewal and colleagues wanted to determine if SPECT/CT, with its more precise anatomic localization, was more useful than conventional planar SPECT in clarifying equivocal findings and in detecting additional abnormalities. They also wanted to see how SPECT/CT would change the initial risk classification of patients, and whether it would result in the need for additional follow-up studies.
The researchers reviewed 148 consecutive patients with thyroid carcinoma who were treated with I-131 at Sloan-Kettering between April 2006 and December 2007. Both planar imaging and SPECT/CT were performed on all 148 patients approximately five days after the therapeutic administration of 1,739 to 8,066 MBq (47 to 218 mCi) of I-131.
Planar images of the body were obtained in the anterior and posterior projections using dual-head gamma cameras (Vertex Plus, Philips Healthcare, Andover, MA) with high-energy general purpose collimators. SPECT/CT images of the neck and chest were obtained on all subjects, with a scan covering the area from the base of the skull to the diaphragm.
Planar versus SPECT/CT
Planar images showed benign findings in 95 (64%) of the 148 patients, equivocal findings in 23 patients (15%), and malignant findings in 30 patients (20%). SPECT/CT confirmed the benign nature of focal I-131 uptake in 82 (86%) of the 95 patients characterized as such on the planar scans, but an additional 12 patients were considered to have malignant disease, while one patient had an equivocal finding.
Among the 23 patients with equivocal findings on the planar scan, 14 patients' findings were characterized as benign, three cases were deemed malignant, and six patients remained equivocal by the SPECT/CT scan.
Among the 30 patients with malignant findings on the planar scan, SPECT/CT confirmed malignant findings in 27 patients (90%), while benign iodine uptake was noted for two patients, along with an equivocal finding in one patient.
SPECT/CT also was significantly more adept at discovering neck node metastases than planar imaging, according to the researchers. In the postsurgical group, planar images showed no I-131 uptake in the neck and no evidence for lymph node metastases among 95 patients, while the SPECT/CT scan confirmed no I-131 uptake in the neck for 83 (87%) of the 95 patients. However, SPECT/CT showed metastatic focal iodine uptake in neck nodes in 12 patients, and there was one case of mild iodine uptake, which remained equivocal on SPECT/CT.
In addition, nine patients had equivocal findings in the lateral neck on planar scans, in which possible nodal uptake was not clearly distinguishable from uptake in the thyroid bed. SPECT/CT findings were deemed negative in three patients, showed focal uptake in neck nodes in five other patients, and remained equivocal in one patient.
Based on those results, lymph node status was changed from stage N0 to N1 or greater in 16 (15%) of the 109 postsurgical patients.
In the 39 patients with suspected thyroid cancer recurrence, 28 showed no evidence of neck nodal disease on planar images. In five (18%) of the 28 patients, SPECT/CT displayed iodine uptake in neck lymph nodes and confirmed the absence of neck disease in the other 23 patients.
Planar images showed the clinical findings in six patients, while SPECT/CT found the equivocal status and classified three patients as negative and three other patients as having focal iodine uptake in neck nodes. The lymph node status was changed from N0 to N1 or greater in eight cases (21%) of the 39 patients in the suspected-recurrence group.
 |
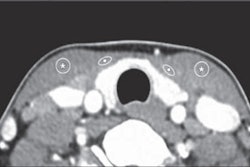
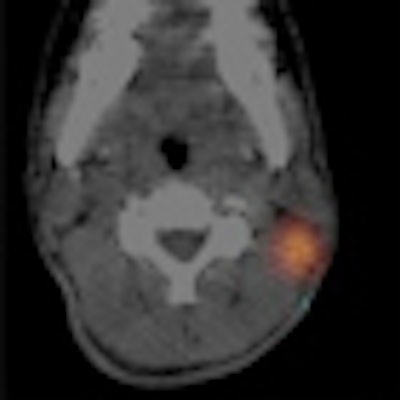
| The planar post-therapy I-131 scan (A) of a 16-year-old boy after a thyroidectomy shows multiple uptake in the neck. In addition, 3D maximum-intensity-projection axial CT, SPECT, and SPECT/CT images (B) show uptake in bilateral lower neck indicating supraclavicular lymphadenopathy. SPECT/CT image (C) also shows iodine-avid left posterior neck node. Images courtesy of the Journal of Nuclear Medicine. |
Follow-up ramifications
Based on the overall results, Grewal and colleagues calculated that an endocrinologist would have requested 90 cross-sectional imaging studies (among 60 of the 148 patients) to clarify findings on planar scans. In comparison, only 29 cross-sectional studies (in 29 patients) would have been requested on the basis of SPECT/CT reporting.
"Therefore, SPECT/CT, compared with medical decision-making based on the planar images alone, avoided 61 cross-sectional imaging studies in 29 patients -- that is, additional imaging studies were avoided in 48% of the patients for whom they would have been considered necessary on the basis of planar scanning alone, or 20% of our entire patient population," the authors wrote.
SPECT/CT should be "strongly considered in intermediate- and high-risk patients after treatment with I-131," Grewal and colleagues recommended. "We now perform SPECT/CT in all post-therapy patients and believe that this has streamlined patient management and avoided additional imaging studies at later time points."
By Wayne Forrest
AuntMinnie.com staff writer
September 3, 2010
Related Reading
Study shows budding turf war for radioiodine procedures, December 29, 2009
SPECT/CT outdoes planar imaging with lymph nodes, January 5, 2009
SPECT/CT once again shows value in bone lesion location, September 18, 2008
SPECT/CT mammography system produces first patient images, July 30, 2008
SPECT/CT offers better bone scan views to enhance treatment, September 21, 2007
Copyright © 2010 AuntMinnie.com