While CT in combination with the Bosniak classification system has been the go-to modality for assessing renal cystic disease, imaging experts are exploring the effectiveness of other modalities for evaluating renal masses. Both ultrasound and MRI were put to the test in two studies presented at the 2003 American Roentgen Ray Society meeting in San Diego.
In the first study, Dr. Richard Barr, Ph.D., and co-authors from St. Elizabeth’s Health Center in Youngstown, OH, reported that contrast-enhanced ultrasound offered several advantages over CT in pinpointing indeterminate masses. In another paper, Dr. Gary Israel and colleagues, including Dr. Morton Bosniak, from New York University Medical Center in New York City, compared CT and MRI and found that the results from the latter modality can result in lesion upgrading, which may alter patient management.
CEUS-based characterization
"I’m here to tell you that ultrasound still exists," Barr said in his introduction. "Renal masses can require several modalities sometimes to characterize lesions, especially indeterminate masses, which remain problematic. We have found that contrast-enhanced ultrasound (CEUS) has several advantages involving these indeterminate masses."
Barr disclosed that his team received research grants from ATL (now part of the ultrasound division of Philips Medical Systems of Andover, MA) and Bristol-Myers Squibb Medical Imaging of North Billerica, MA. In addition, the FDA has approved the two contrast agents used in this study -- Definity by Bristol Myers Squibb and Optison by the Mallinckrodt unit of Tyco Healthcare in Hazelwood, MO -- for cardiac imaging only. Their use in this report was off-label, Barr said.
"Our purpose was to evaluate the long-term follow-up in patients enrolled in several CEUS studies to determine renal masses performed at our center," he explained. Specifically, the group wanted to follow up benign lesions to assess the accuracy of the initial sonographic diagnosis.
Since January 1998, 101 patients with renal masses were included in six clinical trials using different ultrasound techniques: fundamental, color Doppler, and non-linear, contrast-specific techniques.
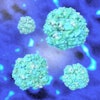
"Ultrasound with contrast has advanced over the years," Barr said. "We now have as many sequences ... as there are in MRI." At the time of these studies, the level of ultrasound technology that his group was using allowed them to inject contrast into a large renal cell carcinoma, and pick out the individual vessels in the cell. Also, the mass enhanced more than the normal renal cortex on ultrasound.
 |
A large renal cell carcinoma on pre-contrast ultrasound (above). After injection of the contrast agents (below), there is enhancement. Individual vessels in this renal cell carcinoma can be picked out; the mass also is enhancing more than the normal renal cortex. "If we increase the mechanical index, we can actually eliminate most of the parenchymal phase and actually look at discrete vessels," Barr said. Images courtesy of Dr. Richard Barr, Ph.D.
 |
Part of the group’s sonographic technique is to increase the mechanical index, eliminate most of the parenchymal phase, and look at discrete vessels.
"This technique is very sensitive and we can actually pick up the difference in blood flow between the medula and the cortex routinely," Barr said. "We find this very helpful looking at pseudotumors because we can see the medullary pyramid within a pseudotumor, and also investigate the blood vessels to show that they are non-irregular and regular."
Lesions with a Bosniak classification of II or III were included in the study, including echogenic solid masses and questionable lesions (e.g. pseudotumors). Follow-up information was gathered between one and four years.
An attempt was made to contact all patients to determine if they had undergone surgery or additional imaging. The patients were subsequently divided into two groups: surgical (renal cell carcinoma, oncocytoma, adenoma, other cancers) and non-surgical (complicated cysts, angiomyolipomas, pyelonephritis). Barr said his group assumed that stability over a two-year period confirmed benign lesions.
"During the study, we diagnosed 30 out of 101 patients as surgical patients; 25 of those had gone to surgery, and of those 24 had renal cell carcinomas. One of those was diagnosed with a complicated cyst. In this patient, there was a very small, enhanced nodule, about 3 mm, on MR. We had one patient with lymphoma and we had one patient that had refused intervention, but had a lesion that enhanced on MR and continued to increase in size. We had three cases of no follow-up. So if we include these as true positives, we diagnosed 26 of the 27 correctly, " Barr said.
 |
A complex cystic mass with a solid portion slightly higher in echogenicity in the cystic component, pre-contrast (above) and post-contrast administration (below). The echogenic component is markedly enhanced on contrast and is a cystic renal carcinoma. Images courtesy of Dr. Richard Barr, Ph.D.
 |
Counting the non-surgical lesions, eight were diagnosed as angiolymphomas; three were diagnosed as pseudotumors; 27 had no change on the follow-up exam for over two years; while the team wasn’t able to get information on 33. Three cases were considered surgical lesions on CEUS, but have not been followed up or undergone surgical treatment.
"We have 26 true positives, 38 true negatives, and one false positive, giving us a sensitivity of 100%, a specificity of 97%, a positive predictive value of 96%, and a negative predictive value of 100%," Barr said.
One of the advantages of ultrasound is that it allows radiologists to differentiate between transitional cells and renal cells, based on their enhancing characteristics.
"CEUS of renal masses has a very high sensitivity and specificity for diagnosing non-surgical lesions," Barr concluded. "With the newer technology, we feel that we can make a distinction between masses. We’re finding that transitional cells do not have the blood volume within them as renal cell carcinoma."
Since completing the study, the group has updated its sonographic technology and technique. "We now have the capability of using pulse sequences that will only show us (echoes) from the contrast. We also have the capability of showing an image without contrast and a combined image of the two, controlling the B-scale and the contrast on top of each other, all done in real time," he said.
MRI upstaging
The purpose of second study, a retrospective analysis, was to "compare the imaging findings at CT and MRI in the evaluation of cystic renal masses and to determine whether the criteria used to classify renal cysts in the Bosniak classification system, based on CT, is applicable to MRI," NYU’s Israel explained.
The study population consisted of 72 masses in 62 patients, based on a search of the institution’s MR database back to 1996. This included "all patients referred for renal MR imaging in which the word ‘cyst’ or ‘cystic neoplasm’ appeared in the acute findings," Israel said.
This information was then cross-referenced with patients who also underwent a dedicated renal CT within one year of the MR. Ten of the 62 patients had both exams performed at outside institutions, the results of which were sent to one of the authors for consultation. The average time interval between both exams was 60 days.
For those exams performed at NYU, the following MR protocol was used on a 1.5-tesla unit with a phased-array coil: 2-D, GRE T1-weighted sequence and SSTSE T2-weighted sequence followed by a fat-suppressed, T1-weighted GRE sequence. Half-Fourier, TSE, and T1-weighted images with and without gadolinium were also obtained.
For CT, images were acquired before and after intravenous contrast administration. The slice collimation was 2.5 to 5 mm, and the scan delay was 90 seconds.
"We first reviewed the CT scan and then reviewed the MRI adjacent to the CT scan. For each lesion, we determined the numbers of septa within it, the thickness of the wall of the septa, whether the lesion enhanced, and gave the lesion a CT Bosniak classification on CT and MR," resolving interpretive differences by consensus, Israel said.
According to the results, 55 of the 72 (or 76% of the time) the CT and the MRI were completely equivalent. In 17 cases (24% of the time), the CT and the MRI did not agree and the MRI results upgraded the Bosniak classification in seven of the lesions.
For the numbers of septa, there was disagreement between the CT and MRI results in eight of the 72 cases, with the Bosniak classification upgraded in two cases on MR.
Israel cited a case of a category II cyst that was seen on CT with a thin wall, no enhancement, no calcifications, and a few hairline-thin septa within the lesion. The corresponding T2-weighted MR images revealed many more hairline-thin septa within this lesion that were still not seen on the CT exam retrospectively. As a result of the MR, the lesion was upgraded to a category IIF.
For the thickness of the wall of the septa, the CT and MR disagreed in five of the cases, resulting in the CT Bosniak classification being upgraded in four cases on MR, Israel stated.
In terms of enhancement, the CT and the MR did not agree in five of the cases. Four of these cases were considered pseudoenhancements on CT; the last case was a cystic mass that contained a neural nodule.
"In summary, we find that CT and MR show similar findings in the majority of suspicious renal masses. In some cases, MR does demonstrate additional septa, wall of septal thickening, or enhancement, which may upgrade a lesion on the Bosniak classification, impacting our patient management," Israel said.
However, he acknowledged that there were limitations to this study. Its drawbacks included a small sample size, the fact that it was a retrospective study utilizing consensus reading, and the lack of standardization for MR and CT exams across all patients.
Still, the group found that the Bosniak renal cyst classification system can also be used with MR studies of most lesions. Israel warned that in some questionable category III lesions on MR -- such as those that could be a category IIF or a category III -- a CT exam should be performed for confirmation of the MR to assist in patient management.
The impact of MR results on questionable cases on CT is key, Israel said.
"For us, it’s really no big harm if the lesion is upgraded from category II to category IIF2F because it’s still a nonoperable lesion and you are basically just following up," he explained. "But if you have a borderline category III lesion on MR, that would be a surgical lesion. We’ve show in some cases that these lesions are category IIF lesions on CT, which would be a non-surgical lesion. We think that has a large impact on patient management, and presently we are using CT to dictate patient management. It’s purely a try to avoid unnecessary operations."
By Shalmali PalAuntMinnie.com staff writer
June 17, 2003
Related Reading
Ultrasound effective in diagnosis, treatment of cystic liver lesions, May 15, 2003
Percutaneous radiofrequency ablation may be an option for solid renal masses, April 21, 2003
Pseudoaneurysm size affects success of thrombin injection with US, April 1, 2003
Radio-frequency ablation effective for many renal cell carcinomas, January 29, 2003
Imaging explores link between kidney failure and atherosclerosis, January 28, 2002
Copyright © 2003 AuntMinnie.com