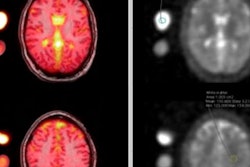
An easy-to-use, automated computer algorithm based on diffusion-tensor MRI (DTI-MRI) scanning is helping to evaluate people with mild traumatic brain injury (TBI). Researchers hope the algorithm will spur more widespread adoption of DTI-MRI in the clinical setting, according to a study published February 1 in Radiology.
The researchers used Shannon entropy, an information and mathematical model designed to look at areas of disorder in complex biological systems, such as the brain. In this case, Shannon entropy works in parallel with DTI-MRI to measure the amount of damage done to white-matter tracts in concussed patients (Radiology, February 1, 2016).
As the amount of information or complexity contained in the data is accumulated by Shannon entropy, the algorithm can determine the degree of injury and its aftereffects. In other words, a healthy brain has high entropy, while a brain with white-matter damage from a mild traumatic trauma may lose some of its complexity and have less entropy.
"The more injury indicated by Shannon entropy, the more likely there could be a longer recovery time," said study co-author Dr. Lea Alhilali, a neuroradiologist with the Barrow Neurological Institute in Phoenix. "It also can better detect in a patient whether he or she is at future risk of neurocognitive issues."
Severe aftereffects
Headaches and migraines are common among people with mild TBI. Post-traumatic migraines have especially high morbidity, are associated with lower neurocognitive test scores, and can aggravate other post-traumatic symptoms that delay recovery, the authors noted.
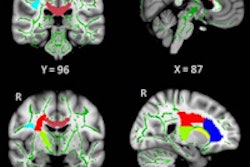
In fact, previous research by Alhilali and colleagues used DTI-MRI to uncover distinct injury patterns in the brains of people with concussion-related depression or anxiety.
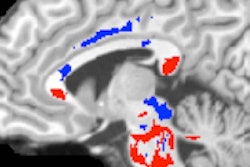
Alhilali explained that many changes occur in the brain after a concussion. The long, thin parts of the nerve cell that send impulses from cell to cell -- known as axons -- may swell, which causes an increase in fractional anisotropy values. If the axons are damaged, fractional anisotropy values will decrease.
"If all you look at is the average of these two different [fractional anisotropy] directions, you don't see a change," she said. "Because Shannon entropy measures how complex the dataset is, if one type of injury moves the fractional anisotropy up and one moves it down, there are two different states, and the Shannon entropy detects the complexity [of the changes]."
That deficiency in DTI-MRI and fractional anisotropy measurements led to the current endeavor.
"We felt that the way radiologists were using diffusion-tensor imaging to analyze water tracts was not sufficient to accurately detect white-matter injuries across the spectrum of concussion patients," Alhilali said. "So, we decided to utilize Shannon entropy to analyze the diffusion-tensor images to see how complex the dataset is."
Targeting mild TBI
The researchers reviewed radiology reports from the University of Pittsburgh Medical Center between January 2006 and January 2014. They found 74 patients with mild TBI, who had a mean age of 18 years (range, 10-47 years). Within this group, 30 patients had experienced a prior concussion and 57 had post-traumatic migraines.
The study also included 22 healthy control subjects and 20 control subjects with migraine headaches. The median time from injury to clinical presentation was 20 days (range, 0-506 days). The most common types of trauma were sports injuries (43 patients, 57%) and motor vehicle accidents (nine patients, 12%).
Diffusion-tensor imaging was performed with a 1.5-tesla MRI scanner (Signa, GE Healthcare) with a standard head coil to acquire fractional anisotropy maps.
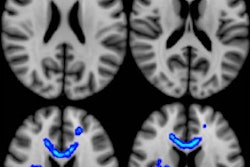
The researchers calculated mean fractional anisotropy values and Shannon entropy scores from DTI total brain fractional anisotropy maps and compared the results between the subject groups. They also analyzed the outcomes of participants with and without post-traumatic migraines.
Mild TBI values
Patients with mild TBI tended to have lower mean fractional anisotropy values (0.379), compared with the healthy control subjects (0.383) and control subjects who experienced migraines (0.382), Alhilali and colleagues found. The mild TBI patients also had significantly lower Shannon entropy scores (0.737) than both the healthy control subjects (0.808) and control subjects with migraines (0.795).
There was no significant difference between healthy control subjects and control subjects with migraines for either fractional anisotropy or Shannon entropy values.
Based on area under the curve (AUC) analysis, Shannon entropy (0.85) outperformed mean fractional anisotropy (0.52) in determining which patients with mild TBI developed post-traumatic migraines (p < 0.001). In addition, patients with Shannon entropy of less than 0.750 were "approximately 16 times more likely to have experienced mild TBI and were three times more likely to develop post-traumatic migraine," the authors wrote.
Post-traumatic migraine was also a factor in determining recovery time. It took patients with migraines a median 51.9 days to recover, compared with a median 39.4 days for those without migraines.
Shannon entropy's future
While Shannon entropy has been used in electrocardiographic (ECG) analysis, it is not well-known or widely used in radiology.
"That is what is very novel about this topic," Alhilali said. "Not only has it never been applied to the imaging of brain white matter, but it also was successful in detecting white-matter injuries."
The authors speculated that Shannon entropy analysis of DTI might help clinicians more accurately diagnose concussion, anticipate patients' symptoms, and predict prognosis in mild TBI.
Alhilali said a benefit of Shannon entropy is that it is easy to use.
"When you do the analysis, which is an easy automated computer algorithm, you get a number, which is very easy for a clinician, radiologist, or researcher to understand," she explained. "A lower number means less complexity in the white matter and a higher number means greater complexity and recovery from mild TBI."
The Barrow Neurological Institute currently has an ongoing study using athletes from Arizona State University to explore factors including accelerometer data, molecular markers, and blood samples, correlating that information with imaging markers of injury.
"We hope that Shannon entropy can be one imaging marker we can use to correlate with mechanical and molecular markers of injury that we detected in other portions of the study," Alhilali said.
She does not think that Shannon entropy will change "the way we analyze diffusion-tensor imaging, because it is a very powerful tool that has yet to find a strong clinical use," she added. "Because there is a great deal of variability in diffusion-tensor imaging measurements, it requires group statistics and comparable analysis that will not be performed by anyone in the clinical setting."
Therefore, she hopes Shannon entropy will help move DTI to the forefront, to be used on individual patients where the results would be more automated and more easily interpreted.
"I think it will help to change the way we analyze diffusion-tensor imaging beyond analyzing injury patterns and mild traumatic brain injury and many other fields in which we use [DTI] for research purposes," she said. "Perhaps Shannon entropy can bring DTI more into the clinical field."