KEY LARGO, FL - Ultrasound can be used as a first-line imaging tool for diagnosing papillomas and other benign breast disorders, allowing clinicians to skip the more invasive galactography exam. Of course, using ultrasound successfully to assess nipple discharge does require the right skill set, said Dr. Thomas Stavros on Tuesday at the Breast Course 2007.
"Before ultrasound-assisted vacuum biopsy, we had to do two galactograms, one for diagnosis using just iodinated contrast agent and one on the day of surgery with a mix of contrast and blue dye to localize the duct for excision by the surgeon," said Stavros. "What we realized is that we could do away with one of the two galactograms. Most of the time, we make the diagnosis with ultrasound and we reserve the galactogram for the day of surgery."
Stavros is the chief of ultrasound and noninvasive vascular services at Radiology Imaging Associates, Medical Imaging of Denver and the Swedish Medical Center in Englewood, CO.
For those who are looking to become proficient in ductal sonography, perform the ultrasound exam right after intraductal lesions have been demonstrated on the galactogram, Stavros said.
"Even if you use galactography as your primary tool, it's good to use ultrasound immediately after the galactogram in case you have to use ultrasound for localization if you're not doing vacuum-assisted biopsy," he said.
In situations in which a diagnosis can be made on galactography alone, ultrasound should still be considered a valuable tool, Stavros added. "We might have a successful galactogram for diagnosis, and then the day (she) comes in for surgery, the patient can't express secretions, so we can't do a galactogram. Ultrasound can save you in those situations as well," he explained.
In terms of sonographic equipment, Stavros recommended that a 1.5D or matrix-array transducer be used to define the ducts all the way to the nipple. He also suggested that the room and the ultrasound gel be warm.
When placing the transducer on the breast, Stavros cautioned against placing too much weight on the soft papillomas and the equally compressible vessels that feed them.
"It's very important that you use proper technique. The transducer is hard, the chest wall is hard, and the duct and vessels are soft. If you hold the transducer up near the end, just the weight of your arm can shut off blood flow so that you can't demonstrate (the ducts and vessels)," Stavros said. He suggested that the transducer be held like a pencil and lifted up slightly to avoid compression.
Another element of proper technique is being able to visualize the entire duct, including the subareolar area and the portion through the nipple, he said. This requires a change in scanning direction, as well as the addition of the following maneuvers: the peripheral compression technique, two-handed compression technique, and rolled nipple technique.
The rolled nipple technique is particularly essential for demonstrating multiple papillomas, echogenic inspissated secretions, and the fibrovascular stalk, which is generally 90° to the duct wall, Stavros said.
"When we scan from straight anterior, we tend not to see the ducts and the nipple well because they are parallel to the beam. We simply have to do maneuvers to tip the nipple on its side. The nipple actually has a lot of internal features…. We can actually follow the ducts all the way through the nipple and through the duct orifice," he said.
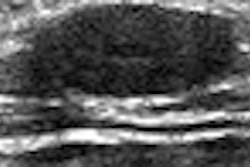
Finally, what to look for on the ultrasound image? Stavros pointed out that intraductal papillomas are commonly, yet inaccurately, referred to as echogenic. Echogenic tissue is fibrous, he said, while papillomas are isoechoic.
"They are the same echogenicity as fat and less echogenic than the duct wall, which is hyperechoic," he said. "You should always demonstrate intraductal papillary lesions in two views: a long axis or radial view, and a short axis or antiradial view."
One major advantage ultrasound has over galactography is that it can show the true length of lesions, he added. "Many times we get what is called the 'duct cutoff sign,' where we see an obstruction at the point of the papillary lesion and we have no idea how long it is. Ultrasound can show you the true length."
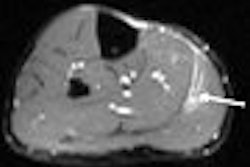
Nonpalpable lesions are one instance in which galactography may be more useful, Stavros acknowledged, but that doesn't rule out the use of ultrasound in cases of suspected ductal ectasia and ductal carcinoma in situ (DCIS). On ultrasound, the following signs can be taken for an increased risk of cancer:
- Hard, suspicious findings
- More than 2-cm expansion of the duct
- Presence of branch ducts
For ductal ectasia in particular, sonography is capable of showing multiple central papillomas in multiple different central ducts, Stavros wrote in the Breast Course syllabus ("The Breast Book 2007").
Overall, Stavros recommended the following imaging course when working with intraductal sonography to assess nipple discharge:
- Schedule both ultrasound and galactography.
- Perform ultrasound exam first.
- If sonogram is positive, continue on to mammotomy.
- If ultrasound offers a definitive diagnosis, no further imaging is required.
- If ultrasound is negative or nonspecific, go on to galactography.
- If the nipple is involved, the problem will require surgical attention.
By Shalmali Pal
AuntMinnie.com staff writer
March 14, 2007
Related Reading
Ultrasound continues to make inroads in breast imaging, February 6, 2007
Papillary breast lesions often underdiagnosed by core-needle biopsy, February 28, 2006
Nipple fluid analysis may help breast cancer evaluation, May 3, 2005
Sonographic findings in focal fibrocystic changes of the breast, May 29, 2002
Copyright © 2007 AuntMinnie.com