
A new quantitative spectral Doppler ultrasound measurement can accurately detect liver transplant hepatic arterial stenosis, offering the potential of reducing the number of unnecessary angiography procedures in these patients, according to research published in the April issue of the Journal of Ultrasound in Medicine.
In a retrospective review of 69 patients who had suspected transplant hepatic arterial stenosis, a team of researchers found that the stenosis index -- a new measure that accounts for the entire spectral Doppler waveform -- was more accurate than traditional quantitative ultrasound metrics for detecting cases of clinically significant stenosis.
 Dr. Sherwin Chan, PhD, from Children's Mercy Hospital.
Dr. Sherwin Chan, PhD, from Children's Mercy Hospital.If the results are generalizable, fewer diagnostic angiography exams would need to be performed for suspected arterial anastomotic stricture in these patients, according to the group.
"The patients would be able to avoid invasive procedures and possible complications, and the healthcare system would be able to save money and/or allocate these resources to more appropriate patients," said pediatric radiologist and senior author Dr. Sherwin Chan, PhD, of Children's Mercy Hospital in Kansas City, MO.
Liver transplant failure
Arterial compromise of the anastomotic site is the leading cause of liver transplant allograft failure, so it's crucial to detect hemodynamically significant allograft arterial stenosis in a timely manner, according to the researchers. However, false-positive results on screening tests -- primarily spectral Doppler ultrasound -- can subject patients to unnecessary invasive procedures such as catheter angiography.
Transplant hepatic arterial patency is typically evaluated via spectral Doppler ultrasound using both qualitative analysis and quantitative measurements, including the pulsatility index and the most commonly used method of resistive index for assessing blood flow downstream from the stenosis. However, these quantitative metrics are calculated using only one or two points in the spectral Doppler waveforms, according to Chan.
"I always thought it was a shame that as radiologists we only used two points of data from a waveform," he told AuntMinnie.com. "The waveform has so much more data included in it that we were just throwing away."
Using the entire waveform
To help, the group developed a technique that uses all points of the waveform to quantitatively detect stenosis, calculated via a stenosis index. They then performed a retrospective study to test their hypothesis that the stenosis index would be more sensitive and specific than the resistive index and pulsatility index for identifying patients with hemodynamically significant transplant hepatic artery stenosis that required intervention (J Ultrasound Med, April 2017, Vol. 36:4, pp. 809-819).
The study included 69 patients who had Doppler ultrasound within 30 days of receiving catheter angiography for suspected transplant hepatic arterial stenosis. The exams were performed by one of 15 sonographers with three to 33 years of experience and were reviewed by attending radiologists, according to the researchers. The waveforms had been recorded with spectral Doppler on one of three different ultrasound machines: HDI 5000 and iU22 (Philips Healthcare) and Elegra (Siemens Healthineers).
The stenosis index was then calculated from each patient's spectral Doppler ultrasound images by obtaining the ratio of the area under the high-frequency signal to the low-frequency index signal in the spectral Doppler. After also calculating the resistive index and pulsatility index, the researchers compared the accuracy of all three metrics using receiver operating characteristic (ROC) analysis.
Higher accuracy
Of the 69 patients, 48 were determined on angiography to have transplant hepatic arterial stenosis requiring intervention; the remaining 21 had no evidence of stenosis on angiography. The researchers found that the stenosis index was lower in patients with transplant hepatic arterial stenosis (1.04 ± 0.20) than in those without stenosis (1.39 ± 0.30). The difference was statistically significant (p < 0.001).
The stenosis index was also more accurate, as determined by the area under the curve (AUC).
| Performance of quantitative metrics for transplant hepatic arterial stenosis | |||||
| Pulsatility index | Resistive index | Stenosis index | |||
| AUC | 0.70 | 0.68 | 0.86 | ||
| Sensitivity | 42% | 96% | 94% | ||
| Specificity | 90% | 29% | 52% | ||
The AUC differences were statistically significant for the stenosis index and the pulsatility index (p = 0.29) and the stenosis index and the resistive index (p = 0.38). The authors concluded that the stenosis index is more accurate than both indexes for detecting transplant hepatic artery stenosis requiring angiographic intervention.
"Although this is a small subset of all patients who undergo screening for transplant hepatic artery stenosis, it is the group that is the most problematic to diagnose," the authors wrote.
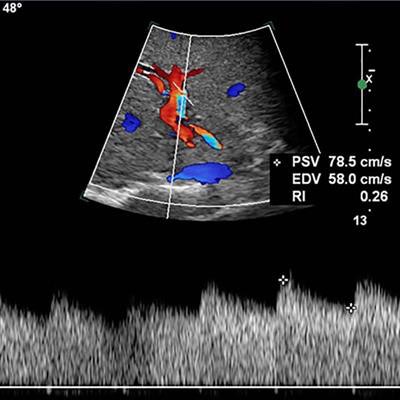
 False-positive case from the resistive index method. Spectral Doppler ultrasound of the right hepatic artery shows a sloping upstroke (A); the resistive index method was low at 0.26, but the stenosis index was high at 1.74. Although there was concern about transplant hepatic arterial stenosis (based on the low resistive index), the digital subtraction celiac angiography (B) showed no flow-limiting stenosis in the hepatic vasculature. As a result, the resistive index method produced a false-positive result. Image courtesy of the Journal of Ultrasound in Medicine.
False-positive case from the resistive index method. Spectral Doppler ultrasound of the right hepatic artery shows a sloping upstroke (A); the resistive index method was low at 0.26, but the stenosis index was high at 1.74. Although there was concern about transplant hepatic arterial stenosis (based on the low resistive index), the digital subtraction celiac angiography (B) showed no flow-limiting stenosis in the hepatic vasculature. As a result, the resistive index method produced a false-positive result. Image courtesy of the Journal of Ultrasound in Medicine.However, it's too early to tell if the stenosis index can replace the resistive index, or whether both indexes should be used together to determine which patients should be referred for angiography, according to the researchers.
"Future studies that compare patients with angiographically proven stenosis versus patients who undergo sonographic screening only, or ultrasound and computed tomography and magnetic resonance imaging, will be useful in assessing a broader patient population," they wrote.
Next steps
Chan noted that the institution is not yet using the stenosis index clinically.
"The processing is not yet automated and requires a lot of radiologist time to do properly," he said.
The group is almost finished, however, with software that can provide automated prediction of stenosis based on its computation of the stenosis index. A member of the research team presented the software this week at the American Medical Informatics Association's 2017 Joint Summits on Translational Science in San Francisco, Chan said.
"We are also working on machine-learning algorithms to improve the prediction even more," he said.

















