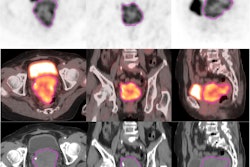
MRI-based machine learning-based nomograms can evaluate postoperative risk factors in cervical cancer patients, a study published October 25 in Academic Radiology has found.
Researchers led by Zhang Yu from the First Affiliated Hospital of Anhui Medical University in China reported that nomograms based on clinical and imaging parameters performed significantly better than MRI alone in assessing cervical cancer risk factors.
“Machine learning-based radiomics have a greater advantage in the prediction of cervical cancer ..., and the combination with incoherent motion diffusion-weighted imaging [IVIM-DWI] and clinical parameters can complement and improve the predictive performance,” Yu and co-authors wrote.
Several risk factors are involved in cervical cancer, which can impact decision-making on treatment strategies. MRI is the go-to imaging method for assessing cervical cancer, but the researchers noted that it can only clarify macroscopic changes. Tissue biopsy and surgical pathology are other methods for assessing this cancer, but these are invasive.
IVIM-DWI is a multi-parametric MRI scanning technique that can reflect the water molecular motion and microcirculatory perfusion of tumors. This shows the pathophysiological state of tumors. Previous research suggests that IVIM-DWI can be applied to a variety of tumors for benign and malignant identification, proliferative potential revelation, recurrence prediction, and prognostic assessment.
Radiomics meanwhile allows for noninvasive analysis, deconstruction, and extraction of many microscopic features of tumors from high-throughput medical imaging.
Yu and colleagues sought to assess the value of machine learning-based radiomics, IVM-DWI, and a combined model in predicting the postoperative risk factors in patients with cervical cancer. They used seven machine-learning methods to determine the radiomics score, which was combined with IVIM-DWI and clinical parameters to build nomograms for predicting the risk factors of cervical cancer.
The team included data from 180 women who were retrospectively analyzed and randomized 2:1 into a training and validation group. It tested the resulting nomograms on the following postoperative risk factors: parametrial infiltration, lymph node metastasis, deep muscle invasion, lymph-vascular space invasion, pathological type, differentiation degree, and Ki-67 expression level.
The researchers found that the area under the curve (AUC) values of the nomograms were significantly higher than those of MRI assessment, though the study did not list p-values.
| Comparison between MRI, nomogram assessment of cervical cancer risk factors | ||
|---|---|---|
| MRI | Nomograms | |
| Parametrial infiltration | 0.868 | 0.981 |
| Lymph node metastasis | 0.639 | 0.848 |
| Deep muscle invasion | 0.78 | 0.896 |
The team also reported that the nomograms performed well in assessing the other included risk factors on training and validation.
For training, this included the following AUC values for training: lymph-vascular space invasion, 0.796; pathological type, 0.854; differentiation degree, 0.806; and Ki-67 expression level, 0.839. For the validation set, the AUC values included the following: lymph-vascular space invasion, 0.84; pathological type, 0.856; differentiation degree, 0.810; and Ki-67 expression level, 0.832.
The study authors suggested that the successful clinical transformation of the model is expected to promote a new model of cervical cancer diagnosis and treatment. This includes helping clarify the choice of surgery and concurrent chemoradiotherapy, reducing ineffective treatments, and improving the prognosis of cervical cancer patients.
“The nomogram model combined with conventional clinical parameters, inflammatory indicators, IVIM-DWI, and radiomics based on machine learning can be used as a practical tool …, providing a basis for risk stratification and individualized treatment of patients with cervical cancer,” the authors wrote.
The full study can be found here.