Palpable ductal carcinoma in situ (DCIS) does not have significant recurrence rates compared to screen-detected DCIS, according to research published December 12 in Surgery Open Science.
A team led by Dr. Nina Balac from the University of Southern California suggested that their findings shed light on DCIS treatment strategies. While patients with palpable DCIS showed more aggressive growth patterns and larger cancers, women in both groups showed similar clinical risk.
"Given concern for overtreatment of DCIS and its implications, we encourage further research aimed at challenging the dogma that palpable DCIS has more adverse tumor biology than screen-detected DCIS," Balac and co-authors wrote.
With greater use of screening mammography comes higher overall detection of DCIS, the investigators explained. Previous research shows that DCIS now accounts for about a quarter of all new breast cancer cases. Most of these are found through imaging, though in rarer cases, they present as palpated masses.
Palpable DCIS can lead to a greater likelihood of the cancer being upgraded to invasive on pathology reports -- which could lead to more surgical interventions and possible overtreatment, the team noted. The group investigated whether palpable DCIS cases show more aggressive disease progress than screen-detected DCIS cases, and if so, what the implications for patient management could be.
The team assessed data from 83 women, 26 of whom had palpable cases and 57 of whom had screen-detected cases. The average follow-up duration was 49.4 months.
The researchers found that 7.7% of palpable cases were upgraded to invasive cancer, compared with 3.5% of screen-detected cases (p = 0.59). They also found no significant differences in local recurrence between both groups (p = 0.55), and no regional or distant recurrence in either group as well.
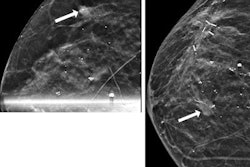
Women with palpable DCIS had significantly larger lesions (p = 0.03). These lesions were more frequently biopsied with ultrasound (p = 0.002) and were significantly tied to ultrasound-guided core needle biopsy, lesion size greater than 2 cm, and comedo pattern.
"This suggests that in the contemporary era, percutaneous core needle biopsy histology may accurately risk stratify lesions and that palpability in stage 0 breast cancer may not portend any worse prognosis," Balac and colleagues wrote.
The study findings suggest that sentinel lymph node biopsy in palpable DCIS cases is unlikely to add to clinical care, and instead may lead to increased morbidity, cost, and difficulty in nodal evaluation if additional breast disease occurs in the future, they concluded.