AuntMinnie.com presents the first in a two-part series on imaging interoperability from Jonathan Shoemaker and Jef Williams of Ascendian Healthcare Consulting.
Perhaps more than any other specialty, radiology has been dramatically affected by the disruption and radical change that has replaced the relative stasis of the healthcare industry. But the imaging interoperability made possible by a vendor-neutral archive (VNA) can help deal with the tumultuous new reality.
Radiology has always been in the vanguard in the early adoption of technology. Long before e-prescribing, enterprise electronic medical records (EMRs), or longitudinal digital patient jackets, radiologists had largely converted from film-based practice to digital imaging. As an early adopter, there is a price of innovation across technology, process, and organization components, but it can be weighed against the long-term benefits gained via maturity, superior patient care, and competitiveness as the healthcare industry changes.
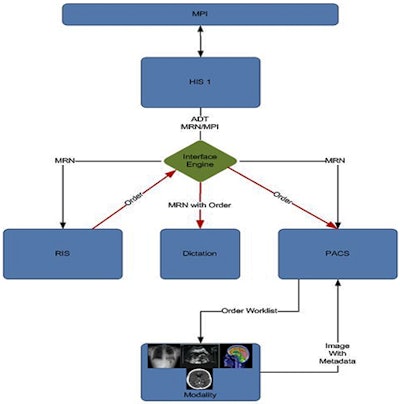
This axiom failed diagnostic imaging and radiologists, however, due primarily to the design, workflow, and short-sightedness of the systems that support their practice: RIS, PACS, and archival systems. The healthcare environment is rapidly changing, but radiology systems still follow a specific chronological flow for creating, storing, and distributing data, as demonstrated in the following figure.
 |
| Single-enterprise solution. Image courtesy of Jonathan Shoemaker and Jef Williams. |
In a single-enterprise environment, or even within a radiology image-centric system, this approach works well. This type of environment is much less optimal, though, as the healthcare paradigm shifts and single systems are replaced with complexity, disparity, and increased interoperability requirements.
The task of simply pushing images from one site (system) to another is no longer sufficient. But the majority of receiving systems do not have the ability to accept images without an order, assign the images to the correct patient with different or missing medical record numbers, and create a report for these images that can be sent correctly back to the originating facility.
An additional factor is the tremendous risk that images could be associated with the incorrect patient. This has left many departments perceiving as the only option the utilization of full-time employees to manually manage and manipulate the data assets to support the deficient departmental systems. This solution is suboptimal, and resulting inefficiencies run counter to cost-containment measures that every healthcare organization is trying to implement to simply remain profitable.
Interim approaches
PACS vendors have countered with patches and interim solutions to help reduce the manual process, including algorithms such as the Integrating the Healthcare Enterprise (IHE) Patient Identifier Cross-Referencing (PIX) integration profile for managing image data. But this does nothing to solve the bigger problem of providing a longitudinal patient jacket or integration back to the originating system.
Healthcare executives are continuously seeking the best practices and solutions to manage image acquisition and data sharing or mergers internally between disparate systems without hiring an army of staff to manage manual processes or retire expensive legacy technology. One of the most common solutions is to consolidate information systems and create a standard platform. This creates standardization but is also expensive and extremely time-consuming. It also does nothing to solve the problem of sharing image data across healthcare systems.
As proclaimed in a recent KLAS report, a fair number of organizations are exploring the emerging technologies available in the market that are being touted as vendor-neutral archives (VNAs).
Vendor-neutral archives
What is a VNA? There are many different flavors of VNAs, and strong business cases can be made for the value of each. What we're referring to here are the approaches that focus not on providing a single static archive for all of an organization's image data, but rather those providing an architecture or interoperability platform that assists the departmental systems in interoperability outside of the department and health system.
PACS are designed to address departmental workflow and are great at accomplishing that task. Asking a PACS to be all things is ludicrous, however, and never really meets all of the required needs while producing a complicated meshwork of rigged solutions.
The insertion of an interoperability platform to create a common archive for all associated clinical systems will help manage storage space but also addresses the significant issue at hand: moving exams and images between disparate systems while supporting the informatics dependencies of the departmental imaging systems (RIS, PACS, dictation) and providing an integration point to enterprise and regional systems (EMR, health information exchange [HIE]).
Breaking out of the borders of the department allows health systems to develop data flow in which information is created first in the subsystem and the results and image links are then populated to the superior systems. This interoperability platform can manage the creation of supporting orders to drive workflow within the department systems regardless of where the originating image was created.
The platform can also act as or integrate into a registry or IHE Cross-Enterprise Document Sharing (XDS) repository to pull, modify, and insert image information into the departmental system while managing and maintaining the storage of those objects based off of rules the departmental system may not be capable of producing or implementing.
An interoperability platform is the key component for rapidly absorbing disparate clinical systems from acquisitions, system replacements, and external HIE sources while supporting the current clinical systems and meeting their needs. The VNA becomes part interoperability content management, part archive, part teleradiology solution, and part results dissemination.
This empowers organizations to manage the tsunami of disparate data they are being asked to manage, store, and move without replacing their clinical systems, which were historically chosen as best-of-breed applications. Many PACS vendors will contest the importance of VNAs, but a VNA provides the client with independence to manage the data outside of the vendor's product limitations.
And, come to think of it, weren't those limitations what created this bitter irony in the first place?
Jef Williams and Jonathan Shoemaker are frequent speakers and writers on healthcare technology topics and enterprise imaging solutions. Jef is a vice president and Jon is a senior consultant at Ascendian Healthcare Consulting.
















