Talcosis:
Clinical:
Talc is hydrous magnesium silicate, but it can be contaminated by other minerals [4]. Inhalational talcosis can be found in miners, millers, rubber workers, and other occupationally exposed groups [4].
Talcosis is also seen in I.V. drug users secondary to the
intravenous abuse of crushed oral medications [5]. Numerous tiny
particles of talc become lodged in the pulmonary vessels/capillary
bed and migrate into
the interstitium [6]. The disorder represents a foreign body
granulomatous reaction to the talc particles which can
progress to interstitial fibrosis. Talc also contains magnesium
silicate (similar to
asbestos) and this may be the etiologic agent that elicits the
inflammatory response.
Patients experience progressive dyspnea and symptoms resembling chronic obstructive pulmonary disease [1]. Patients can also develop pulmonary arterial hypertension if the emboli are widespread and incite a pronounced foreign body granulomatous response [2]. A talc retinopathy is seen in 80% of cases. Talc crystals are birefringent under polarized light.
X-ray:
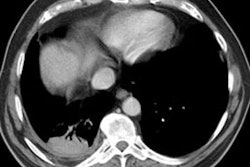
Findings of inhalational talcosis on CXR are small, nodular opacities in all lung zones and CT showing diffusely distributed 1-2 mm centrilobular nodules [4]. Larger opacities (round or irregular) over 1 cm are common and may be of high attenuation [4]. Other common findings include septal and subpleural lines and ground-glass opacities [4]. Slight lymph node enlargement of increased attenuation are also common [4].
In IV talcosis on CXR, initially there are widespread 2-3mm
well-defined nodules which coalesce over
time producing homogeneous opacities. The disorder mimics
progressive massive fibrosis
seen in silicosis or coal worker's pneumoconiosis, but tends to
affect middle lung zones.
Diaphragmatic calcifications similar to those seen in asbestosis
may also be seen.
Lymphadenopathy is rare [3].
On CT, findings include a diffuse fine micronodular/granular centrilobular pattern, ground glass attenuation, and lower lobe panlobular emphysematous changes [1]. Conglomerate masses are uncommon and typically related to inhalation of talc particles [6]. These masses frequently have high attenuation values resembling calcium [1].
REFERENCES:
(1) AJR 2000; Ward S, et al. Talcosis
associated with IV abuse of
oral medications: CT findings. 174: 789-793
(2) Radiographics 2000; Frazier AA, et al. From the archives of the AFIP. Pulmonary vasculature: Hypertension and infarction. 20: 491-524
(3) AJR 2000; Rossi SE, et al. Nonthrombotic pulmonary emboli. 174: 1499-1508
(4) AJR 2007; Akira M, et al. Inhalational talc pneumoconiosis: radiographic and CT findings in 14 patients. 188: 326-333
(5) Radiographics 2007; Restrepo CS, et al. Pulmonary
complications from cocaine and cocaine-based substances: imaging
manifestations. 27: 941-956
(6) Radiographics 2020; Naeem M, et al. Noninfectious granulomatous diseases of the chest. 40: 1003-1019