Radiographics 2002 Oct;22 Spec No:S167-84
Asbestos: when the dust settles an imaging review of asbestos-related
disease.
Roach HD, Davies GJ, Attanoos R, Crane M, Adams H, Phillips S.
Asbestos-related neoplastic and nonneoplastic diseases of the lungs and pleura
range from pleural effusion and pleural plaques to lung cancer and malignant
mesothelioma. Pleural effusions are typically hemorrhagic exudates of mixed
cellularity but do not typically contain asbestos bodies. The classic
distribution of pleural plaques seen on chest radiographs is the posterolateral
chest wall between the seventh and tenth ribs, lateral chest wall between the
sixth and ninth ribs, the dome of the diaphragm, and the mediastinal pleura.
Computed tomographic (CT) findings support this distribution but also show
anterior and paravertebral plaques not well shown at chest radiography. Imaging
features of diffuse pleural thickening include a continuous sheet, often
involving the costophrenic angles and apices, that rarely calcifies. The typical
CT features of round atelectasis are of a round or oval mass that abuts the
pleura, a "comet tail" of bronchovascular structures going into the
mass, and thickening of the adjacent pleura. Features of asbestosis on chest
radiographs include ground-glass opacification, small nodular opacities,
"shaggy" cardiac silhouette, and ill-defined diaphragmatic contours.
CT, however, is more sensitive in their detection. Chest radiography in patients
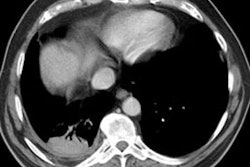
with malignant mesothelioma may show an effusion, pleural thickening, and as the
tumor progresses, a more lobulated outline. CT can help identify the disease in
its early stages. Asbestos-related cancers can occur anywhere in the lungs.
Recognition of the clinical, radiologic, and pathologic features of these
diseases will be important for some years to come.