Thoracic Outlet Syndrome
Clinical:
The thoracic outlet syndrome (TOS) consists of three separate
compartments- the interscalene triangle, the costoclavicular
space, and
the retropectoralis minor space [1]. Thoracic outlet syndrome
occurs
secondary to compression of the neurovascular structures crossing
the
thoracic outlet [1]. It is caused by the impingement of the
brachial
plexus nerves, subclavian artery, and subclavian vein in the area
just
above the 1st rib and behind the clavicle [2].
Affected patients are generally 20-40 years in age and there is a
female predominance (4:1) [1] although other authors indicate no
sex predilection [3]. More than
90% of cases present with neurologic symptoms, whereas fewer than
10%
of patients have vascular only or combined neurogenic and vascular
symptoms [2]. The symptoms consist of pain, numbness,
tingling, and weakness of the upper extremity that is exacerbated
by
activity requiring elevation or sustained use of the arm [1].The
end stage of neurogenic TOS can result in Gilliatt-Sumner hand in
which there is atrophy of the hand muscles, as well as
hyperesthesia in the ulnar and medial antebrachial cutaneous
distributions with normal median nerve sensation [3].
Venous TOS is the second most common form [3]. The typical site
of subclavian vein compression is at the level of the
costoclavicular space between the first rib, subclavius muscle,
and clavicle [3]. Most patients present with spontaneous
axillosubclavian thrombosis (Paget-von Schrotter syndrome),
although symptoms of intermittent venous compression in the
absence of thrombosis is also seen (McCleery syndrome) [3].
Arterial TOS is the rarest form accounting for less than 3% of
cases and most affected patients are young and otherwise healthy
and report a history of vigorous use of the arm in occupational or
recreational activities [3]. Arterial TOS is almost always
associated with an underlying bone abnormality (cervical rib or
anomalous first rib) [3]. Arterial TOS classically presents with
symptoms of distal ischemia including weakness, cold limb, and
pain [3]. Patients with vascular symptoms warrant early
recognition
and treatment to avoid devastating complications such as pulmonary
embolism, gangrene of the hand (associated with Paget-von
Schrotter syndrome), digital ischemia, or stroke due
to emboli originating in the subclavian artery [2]. Stent
placement is not recommended as stent placement alone without
surgical intervention generally fails and the presence of the
stent can limit options for vein reconstruction after stent
failure [3].
Antomic variations that can increase the risk for thoracic outlet
syndrome include a cervical rib or an elongated transverse process
of
C7 [1]. Thin women with poor posture and weak muscle support also
seem
to be predisposed to TOS [1]. Most patients also have a history of
trauma (such as a hyper-extension neck injury) or a work related
repetitive movement [3].
X-ray:
Cervical ribs occur in up to 6% of individuals and are twice as
common in women [3]. Cervical ribs are commonly incomplete (70% of
cases) and usually have a thick ligament extending from their tip
to the first rib [3]. Complete cervical ribs account for 30% of
cases and attach to the normal first rib by fusion or by forming a
joint [3]. Most patients with cervical ribs are asymptomatic, but
an increased prevalence of cervical ribs has been noted in
patients with TOS [3].
An elongated C7 transverse process is more common than a cervical
rib (up to 25% of individuals) and is defined as extending
laterally beyond the transverse process of T1 [3].
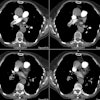
CT angiography can demonstrate vascular compression and the
adjacent
anatomic structures [1]. Imaging should be performed with the arms
alongside the body and then with the arms elevated [1]. Contrast
should
be injected on the contralateral side [1]. Arterial compression is
easily identified, however, venous compression is very difficult
to
discriminate as it is frequently seen in asymptomatic subjects
when the
arms are elevated (seen in over 50% of asymptomatic patients)
[1,3]. Venous thrombosis, focal fixed subclavian vein stenosis,
and collateral circulation are
objective evidence for venous TOS [1].
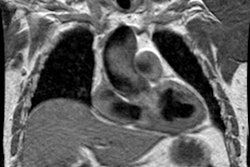
On MR, findings suggestive of neurogenic TOS include edema in the
brachial plexus or loss of the fat surrounding the brachial plexus
with abduction [3].
REFERENCES:
(1) Radiographics 2006; Demondion X, et al. Imaging assessment of
thoracic outlet syndrome. 26: 1735-1750
(2) AJR 2012; Ersoy H, et al. Vascular thoracic outlet syndrome:
protocol design and diagnostic value of contrast-enhanced 3D MR
angiography and equilibrium phase imaging on 1.5- and 3-T MRI
scanners.
198: 1180-1187
(3) Radiographcis 2016; Raptis CA, et al. Imaging of the patient
with thoracic outlet syndrome. 36: 984-1000